Das könnte Ihnen auch gefallen
- Biologic Width & Emergence ProfileDokument33 SeitenBiologic Width & Emergence ProfileNirav RathodNoch keine Bewertungen
- Biologic Width and Its Clinical ImplicationsDokument30 SeitenBiologic Width and Its Clinical ImplicationsNeetu Jha50% (2)
- Crown LengtheningDokument12 SeitenCrown LengtheningKesavaa Vasuthaven100% (1)
- Treatment Planning Single Maxillary Anterior Implants for DentistsVon EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNoch keine Bewertungen
- THE ORTHODONTIC ROADMAP: GUIDELINES FOR THE DIAGNOSIS AND TREATMENT OF ORTHODONTIC MALOCCLUSIONSVon EverandTHE ORTHODONTIC ROADMAP: GUIDELINES FOR THE DIAGNOSIS AND TREATMENT OF ORTHODONTIC MALOCCLUSIONSNoch keine Bewertungen
- Dental Implant Treatment Planning for New Dentists Starting Implant TherapyVon EverandDental Implant Treatment Planning for New Dentists Starting Implant TherapyBewertung: 4 von 5 Sternen4/5 (1)
- Supra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsVon EverandSupra-Gingival Minimally Invasive Dentistry: A Healthier Approach to Esthetic RestorationsBewertung: 5 von 5 Sternen5/5 (1)
- Recent Advances in Procthodontics - LD (AMAR)Dokument102 SeitenRecent Advances in Procthodontics - LD (AMAR)Archana PanwarNoch keine Bewertungen
- Gingivally Approaching Clasp - PedagogyDokument35 SeitenGingivally Approaching Clasp - PedagogyNiaz AhammedNoch keine Bewertungen
- Precision AttachmentDokument33 SeitenPrecision AttachmentLucky SinganamalaNoch keine Bewertungen
- Implant OcclusionDokument52 SeitenImplant OcclusionElango25489100% (3)
- Denture Sequelae: Common Side Effects of Wearing Complete DenturesDokument58 SeitenDenture Sequelae: Common Side Effects of Wearing Complete Denturesaayush100% (2)
- Selective GrindingDokument4 SeitenSelective GrindingDentist HereNoch keine Bewertungen
- Periodontal Considerations in RPDDokument69 SeitenPeriodontal Considerations in RPDPuneet Pandher100% (2)
- 2 Partial Denture Design FayadDokument53 Seiten2 Partial Denture Design FayadMostafa Fayad100% (3)
- Occlusal Consideration in Implant ProsthesisDokument59 SeitenOcclusal Consideration in Implant ProsthesisDrFarha NazNoch keine Bewertungen
- Swing Lock Partial DentureDokument22 SeitenSwing Lock Partial DentureSanNoch keine Bewertungen
- Implantfailurepankajfinal 160120192933Dokument104 SeitenImplantfailurepankajfinal 160120192933DrIbrahimShaikh100% (1)
- Balanced Occlusion: Dr. Rakshith HegdeDokument104 SeitenBalanced Occlusion: Dr. Rakshith HegdePragya Jain67% (3)
- Review of Dental ImplantDokument10 SeitenReview of Dental Implantmar100% (1)
- Periodontal Surgery Objectives and TechniquesDokument67 SeitenPeriodontal Surgery Objectives and TechniquesShabeer Ali Abdul SalamNoch keine Bewertungen
- Prostho Rehabilitation - HypodontiaDokument24 SeitenProstho Rehabilitation - HypodontiaAmniAzmiNoch keine Bewertungen
- Recording Centric Jaw Relation - Review ArticleDokument7 SeitenRecording Centric Jaw Relation - Review ArticleDilesh PradhanNoch keine Bewertungen
- Mandibular MovementsDokument110 SeitenMandibular MovementsNeha Aggarwal100% (1)
- Recent advances in dental implant imaging and placement techniquesDokument3 SeitenRecent advances in dental implant imaging and placement techniquesvinayak shuklaNoch keine Bewertungen
- Esthetics in FPD Seminaar 7Dokument71 SeitenEsthetics in FPD Seminaar 7DrFarha Naz100% (1)
- Interdisciplinary Seminar - CLPDokument80 SeitenInterdisciplinary Seminar - CLPSharanya Bose100% (1)
- Anterior Implant EstheticsDokument9 SeitenAnterior Implant EstheticsRatih Cynthia100% (1)
- Provisional Restoration in FPDDokument45 SeitenProvisional Restoration in FPDrejipg100% (1)
- Retention in Complete DentureDokument53 SeitenRetention in Complete DentureVikas Aggarwal67% (3)
- Management of Residual Ridge Reduction (RRR)Dokument23 SeitenManagement of Residual Ridge Reduction (RRR)drmohitmalviyaNoch keine Bewertungen
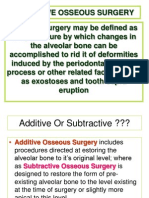
- Resective Osseous Surgery - Oral SurgeryDokument28 SeitenResective Osseous Surgery - Oral SurgeryCristina DağyudanNoch keine Bewertungen
- Presentasi Maxillofacial ProsthesisDokument35 SeitenPresentasi Maxillofacial ProsthesisImeLdaMargaRethaNoch keine Bewertungen
- Biologic WidthDokument26 SeitenBiologic Widthbhasalepooja67% (3)
- Smile Analysis: Staff Incharge Dr. A. SrikanthDokument124 SeitenSmile Analysis: Staff Incharge Dr. A. SrikanthLikhitaNoch keine Bewertungen
- OBTURATORSDokument69 SeitenOBTURATORSSecret OriginsNoch keine Bewertungen
- OCCLUSION IN FPD AND IMPLANTSDokument68 SeitenOCCLUSION IN FPD AND IMPLANTSDRSH100% (1)
- Perio Restorative Inter Relationship (Perio)Dokument44 SeitenPerio Restorative Inter Relationship (Perio)FourthMolar.com75% (4)
- of Mouth PreparationDokument106 Seitenof Mouth PreparationDrSweta Gandhi100% (2)
- Steps of Construction Complete DentureDokument31 SeitenSteps of Construction Complete DentureShanna Hosein0% (1)
- Patients Complaints Following Partial Denture InsertionDokument50 SeitenPatients Complaints Following Partial Denture InsertionHector Sa50% (2)
- Basic Implant SurgeryDokument72 SeitenBasic Implant SurgeryKandiwapa100% (2)
- Overdenture Presentation PDFDokument19 SeitenOverdenture Presentation PDFAjay Mehta100% (1)
- Prostho-Perio-Restorative Interrelationship ADokument6 SeitenProstho-Perio-Restorative Interrelationship AAlipio GarcíaNoch keine Bewertungen
- Distal ExtensionDokument110 SeitenDistal ExtensionParmod GuliaNoch keine Bewertungen
- The Distal Extension Base Denture.1 PDFDokument5 SeitenThe Distal Extension Base Denture.1 PDFenlighten070% (1)
- ObturatorsDokument28 SeitenObturatorsDianne Mamaid100% (1)
- Acute Necrotizing Ulcerative Gingivitis: (ANUG)Dokument36 SeitenAcute Necrotizing Ulcerative Gingivitis: (ANUG)Louis HutahaeanNoch keine Bewertungen
- Border Molding in Complete DentureDokument40 SeitenBorder Molding in Complete DentureVishnu S Pattath0% (1)
- Marburg Double Crown System For Partial DentureDokument10 SeitenMarburg Double Crown System For Partial DentureAhmad Shoeib100% (1)
- Management of Highly Resorbed Mandibular RidgeDokument11 SeitenManagement of Highly Resorbed Mandibular RidgeAamir BugtiNoch keine Bewertungen
- Scientic Rationale For Dental Implant DesignDokument34 SeitenScientic Rationale For Dental Implant DesignvikramNoch keine Bewertungen
- Objectives of Impression MakingDokument24 SeitenObjectives of Impression MakingMadiha ZufaNoch keine Bewertungen
- Esthetics IllusionDokument8 SeitenEsthetics IllusionAmar BhochhibhoyaNoch keine Bewertungen
- Dr. Omkar Shetty - ProsthoDokument7 SeitenDr. Omkar Shetty - ProsthoSyed NooraniNoch keine Bewertungen
- Preventive ProsthodonticsDokument11 SeitenPreventive Prosthodonticssiddu76100% (1)
- Essential OilDokument1 SeiteEssential OilRohit RaiNoch keine Bewertungen
- Avveolar Bone Loss DeterminationDokument17 SeitenAvveolar Bone Loss DeterminationRohit RaiNoch keine Bewertungen
- Blood InvestigationDokument70 SeitenBlood InvestigationRohit RaiNoch keine Bewertungen
- Intermediate PlaxusDokument20 SeitenIntermediate PlaxusRohit RaiNoch keine Bewertungen
- Bone CellDokument47 SeitenBone CellRohit RaiNoch keine Bewertungen
- Medical EmergencyDokument99 SeitenMedical EmergencyRohit RaiNoch keine Bewertungen
- Dentogingival UnitDokument4 SeitenDentogingival UnitRohit RaiNoch keine Bewertungen
- Tooth MobilityDokument19 SeitenTooth MobilityRohit RaiNoch keine Bewertungen
- Emotional Influences On Food Choice Sensory, Physiological andDokument9 SeitenEmotional Influences On Food Choice Sensory, Physiological andpanda_pandita22Noch keine Bewertungen
- Cardiovascular Physiology Case 9Dokument50 SeitenCardiovascular Physiology Case 9Kim AcostaNoch keine Bewertungen
- Pre Conference Final ProgDokument2 SeitenPre Conference Final ProgkeithlyndNoch keine Bewertungen
- Zocor (Simvastatin)Dokument3 SeitenZocor (Simvastatin)E100% (1)
- Thyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Dokument11 SeitenThyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Vaishnavi SheteNoch keine Bewertungen
- Hi Tech International GroupDokument2 SeitenHi Tech International Grouphtig89Noch keine Bewertungen
- Journal Hydrodynamic Theory by Brnnstrm1986Dokument5 SeitenJournal Hydrodynamic Theory by Brnnstrm1986Fifth TsuchikageNoch keine Bewertungen
- 3.pleural Effusion Imaging - Overview, Radiography, Computed TomographyDokument32 Seiten3.pleural Effusion Imaging - Overview, Radiography, Computed TomographyAchmadRizaNoch keine Bewertungen
- Obesity Exercise PrescriptionDokument34 SeitenObesity Exercise Prescriptionkhushbu88% (8)
- ResumeDokument7 SeitenResumeRonald Fuéntes EndómaNoch keine Bewertungen
- JK SCIENCE: Verrucous Carcinoma of the Mobile TongueDokument3 SeitenJK SCIENCE: Verrucous Carcinoma of the Mobile TonguedarsunaddictedNoch keine Bewertungen
- Staph and Strep Lab Report BMS 501Dokument2 SeitenStaph and Strep Lab Report BMS 501aruiz93Noch keine Bewertungen
- Big Book Sponsorship - The Twelve Step Program - Big Book Guide - 4-Hour-12-StepsDokument30 SeitenBig Book Sponsorship - The Twelve Step Program - Big Book Guide - 4-Hour-12-StepscafegrNoch keine Bewertungen
- Administering Corticosteroids in Neurologic Diseases3724Dokument12 SeitenAdministering Corticosteroids in Neurologic Diseases3724Carmen BritoNoch keine Bewertungen
- 2014 Body Code Client Information PDFDokument7 Seiten2014 Body Code Client Information PDFkrug100% (1)
- Integrating Modern Dermatology and AyurvedaDokument25 SeitenIntegrating Modern Dermatology and AyurvedachandusgNoch keine Bewertungen
- List of Doctors by SpecialtyDokument6 SeitenList of Doctors by Specialtykaushal shahNoch keine Bewertungen
- HypothyroidismfinalpptDokument91 SeitenHypothyroidismfinalpptswathi bsNoch keine Bewertungen
- Planes Systems OrganizationDokument36 SeitenPlanes Systems OrganizationR. EssoNoch keine Bewertungen
- Ayushman Bharat - KailashDokument11 SeitenAyushman Bharat - KailashKailash NagarNoch keine Bewertungen
- IV. Physical Assessment Norms Actual Findings Interpretation and Analysis General Appearance Posture / GaitDokument9 SeitenIV. Physical Assessment Norms Actual Findings Interpretation and Analysis General Appearance Posture / GaitMarianne_Miraflo_154Noch keine Bewertungen
- Medicine in Situ Panchen TraditionDokument28 SeitenMedicine in Situ Panchen TraditionJigdrel77Noch keine Bewertungen
- Joint InfectionsDokument10 SeitenJoint InfectionsJPNoch keine Bewertungen
- Abigail BDokument3 SeitenAbigail BbjhilarioNoch keine Bewertungen
- BSN 4A Group 5 Nigerian AmericanDokument39 SeitenBSN 4A Group 5 Nigerian AmericanAngelie PantajoNoch keine Bewertungen
- PG Physician Guide 03 Eng1Dokument88 SeitenPG Physician Guide 03 Eng1hüseyin vururNoch keine Bewertungen
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Dokument5 SeitenList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesNoch keine Bewertungen
- This Just In!: Queen Pin Carla!Dokument10 SeitenThis Just In!: Queen Pin Carla!BS Central, Inc. "The Buzz"Noch keine Bewertungen
- MammographyDokument27 SeitenMammographyRohmatullah Anas100% (1)
- Features FNCP:: Health Nursing ProblemsDokument12 SeitenFeatures FNCP:: Health Nursing Problemsrodeliza100% (2)