Das könnte Ihnen auch gefallen
- Drummond Methods For The Economic Evaluation of Health Care Programmes PDFDokument461 SeitenDrummond Methods For The Economic Evaluation of Health Care Programmes PDFGerman Camilo Viracacha Lopez80% (10)
- PATIENT DETAILSDokument8 SeitenPATIENT DETAILSKaarthigan RamaiahNoch keine Bewertungen
- Autism AssessmentDokument37 SeitenAutism AssessmentRafael Martins94% (16)
- Pelvic MassesDokument15 SeitenPelvic MassesJulia kwapeNoch keine Bewertungen
- Hypnotherapy Scripts 6 Steve G Jones Ebook PDFDokument66 SeitenHypnotherapy Scripts 6 Steve G Jones Ebook PDFjohannes2212100% (10)
- Adult Early Warning Score Observation Chart For High Dependency UnitDokument2 SeitenAdult Early Warning Score Observation Chart For High Dependency Unitalexips50% (2)
- Sarawuth Noppiboon ID 56070700020 BioPhEPs SystemsDokument5 SeitenSarawuth Noppiboon ID 56070700020 BioPhEPs SystemsSarawuth NoppiboonNoch keine Bewertungen
- Appendicitis SampleDokument15 SeitenAppendicitis SampleChiqui Lao DumanhugNoch keine Bewertungen
- Peptic UlcerDokument59 SeitenPeptic UlcerfloramaeyecyecNoch keine Bewertungen
- Powerpoint: ComplicationsDokument50 SeitenPowerpoint: Complicationsj.doe.hex_8750% (2)
- intestinal obstruction 2Dokument46 Seitenintestinal obstruction 2Lawrence WanderiNoch keine Bewertungen
- Ms AJCRS 99757Dokument6 SeitenMs AJCRS 99757Cesar DominguezNoch keine Bewertungen
- Gossypiboma - A Rare Cause of Gastric Outlet ObstructionDokument3 SeitenGossypiboma - A Rare Cause of Gastric Outlet ObstructionJuniper PublishersNoch keine Bewertungen
- Chapter 83. Bowel Obstruction Introduction and EpidemiologyDokument2 SeitenChapter 83. Bowel Obstruction Introduction and EpidemiologylotskiNoch keine Bewertungen
- Intestinal ObstructionDokument13 SeitenIntestinal Obstructionsantosh kumarNoch keine Bewertungen
- Visayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieDokument43 SeitenVisayas Community Medical Center Department of Surgery: Curan, Jan Kleen Ediza, Janseen Tortugo, Andrea MarieJanseen EdizaNoch keine Bewertungen
- Powerpoint: Colorectal Surgical DiseasesDokument74 SeitenPowerpoint: Colorectal Surgical Diseasesj.doe.hex_87100% (1)
- Paralytic Ileus Complication of Acute Appendicitis Dudley, M.DDokument6 SeitenParalytic Ileus Complication of Acute Appendicitis Dudley, M.Dandre nicholasNoch keine Bewertungen
- Acute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Dokument63 SeitenAcute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Rumana IslamNoch keine Bewertungen
- Examination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaDokument29 SeitenExamination of Intestinal Obstruction, Acute Abdomen and Acute Appendicitis - Eugh & BwembyaForeighn97Noch keine Bewertungen
- APPENDECITISDokument5 SeitenAPPENDECITISfxbukenyaNoch keine Bewertungen
- Pub+Enterite+Necrozante+Iasi UnlockedDokument5 SeitenPub+Enterite+Necrozante+Iasi UnlockedlPiNGUSlNoch keine Bewertungen
- Suppurative AppendicitisDokument2 SeitenSuppurative Appendicitisreanne_davidNoch keine Bewertungen
- Case Study Appendicitis: Gian Carlo P. Hijosa BSN 3Y1-10 Ms. Catherine J. CabreraDokument10 SeitenCase Study Appendicitis: Gian Carlo P. Hijosa BSN 3Y1-10 Ms. Catherine J. CabreraGiannie Carlonnie HijosaNoch keine Bewertungen
- What Is An Acute AbdomenDokument112 SeitenWhat Is An Acute AbdomenLavasa SharmaNoch keine Bewertungen
- Peptic Ulcer: by Dr.A.Vijay Anand Dept. of SurgeryDokument79 SeitenPeptic Ulcer: by Dr.A.Vijay Anand Dept. of Surgeryvjanand07Noch keine Bewertungen
- Pancreatitis Ercp Pain Amylase Lipase ErcpDokument24 SeitenPancreatitis Ercp Pain Amylase Lipase ErcpPerplexed CeleryNoch keine Bewertungen
- Neonatal Acute Abdomen. 7th YrDokument54 SeitenNeonatal Acute Abdomen. 7th YrFreeburn SimunchembuNoch keine Bewertungen
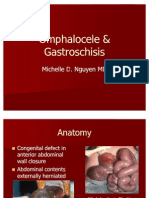
- Omphalocele GastroschisisDokument12 SeitenOmphalocele GastroschisisOlivelhynn Bernaldo100% (1)
- CPC PancreatitisDokument67 SeitenCPC PancreatitisM. Baidar SaeedNoch keine Bewertungen
- Chronic Gastric Volvulus With Diaphragmatic 2024 International Journal of SDokument5 SeitenChronic Gastric Volvulus With Diaphragmatic 2024 International Journal of SRonald QuezadaNoch keine Bewertungen
- Inflammatory Bowel DiseaseDokument59 SeitenInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiNoch keine Bewertungen
- Symptoms and Treatment of Gallstone DiseaseDokument6 SeitenSymptoms and Treatment of Gallstone DiseaseJoharaNoch keine Bewertungen
- Early Enteral NutritionDokument55 SeitenEarly Enteral NutritionAdya ArradikhaNoch keine Bewertungen
- Vovulusoriginal Copy 121028055752 Phpapp01Dokument37 SeitenVovulusoriginal Copy 121028055752 Phpapp01Bheru LalNoch keine Bewertungen
- Clinical aPPROACH TO Acute Abdomen: Dr. J. S. LambaDokument27 SeitenClinical aPPROACH TO Acute Abdomen: Dr. J. S. LambaPushpanjali Crosslay HospitalNoch keine Bewertungen
- Acute Intestinal Failure.11Dokument6 SeitenAcute Intestinal Failure.11albimar239512Noch keine Bewertungen
- 01 Volvulus Sigmoid ScripcariuDokument6 Seiten01 Volvulus Sigmoid ScripcariuHellen RaczNoch keine Bewertungen
- Necrotizing Enterocolitis: Reproduction System 2010Dokument39 SeitenNecrotizing Enterocolitis: Reproduction System 2010Anonymous Af24L7Noch keine Bewertungen
- Complications of AppendicitisDokument34 SeitenComplications of Appendicitisr_ramsewak7Noch keine Bewertungen
- Dr. Pankaj Kumar Assistant Professor Surgical GastroenterologyDokument39 SeitenDr. Pankaj Kumar Assistant Professor Surgical GastroenterologyIlham Suryo Wibowo AntonoNoch keine Bewertungen
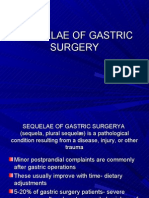
- Powerpoint: Sequelae of Gastric SurgeryDokument86 SeitenPowerpoint: Sequelae of Gastric Surgeryj.doe.hex_87Noch keine Bewertungen
- Gastric Perforation in The Newborn: Ai-Xuan Le Holterman, M.DDokument23 SeitenGastric Perforation in The Newborn: Ai-Xuan Le Holterman, M.Dpldhy2004Noch keine Bewertungen
- Diagnostics Serum Lab Studies:: 105 - Module G GastrointestinalDokument17 SeitenDiagnostics Serum Lab Studies:: 105 - Module G Gastrointestinalamanda081106Noch keine Bewertungen
- SN 212Dokument59 SeitenSN 212Daroo D.TNoch keine Bewertungen
- Powerpoint: Lecture 10, The Small Bowel and AppendixDokument89 SeitenPowerpoint: Lecture 10, The Small Bowel and Appendixj.doe.hex_87100% (1)
- CholecystitisDokument2 SeitenCholecystitisSierrah SlaughterNoch keine Bewertungen
- Colon 2Dokument56 SeitenColon 2EnydLaRejNoch keine Bewertungen
- 03 150427073915 Conversion Gate01Dokument52 Seiten03 150427073915 Conversion Gate01maithamNoch keine Bewertungen
- Diverticular Disease: Causes, Symptoms and TreatmentDokument27 SeitenDiverticular Disease: Causes, Symptoms and TreatmentHotstar serials, cricket LiveNoch keine Bewertungen
- Gastric Volvulus With Hiatal Hernia in A Young Male A Case ReportDokument5 SeitenGastric Volvulus With Hiatal Hernia in A Young Male A Case ReportAthenaeum Scientific PublishersNoch keine Bewertungen
- Case Report: The Combination of Gastroschisis, Jejunal Atresia, and Colonic Atresia in A NewbornDokument5 SeitenCase Report: The Combination of Gastroschisis, Jejunal Atresia, and Colonic Atresia in A NewbornAnonymous PmfX227Noch keine Bewertungen
- Intestinal ObstructionDokument9 SeitenIntestinal ObstructionHamss AhmedNoch keine Bewertungen
- DYSPHAGIADokument76 SeitenDYSPHAGIASaurabh AgarwalNoch keine Bewertungen
- Acute AbdomenDokument7 SeitenAcute AbdomenStanley MwendaNoch keine Bewertungen
- Chapter 4 5 Digestive - RespiDokument8 SeitenChapter 4 5 Digestive - RespiALYSSA PACHECONoch keine Bewertungen
- PeritonitisDokument4 SeitenPeritonitisAlthof SonaNoch keine Bewertungen
- Data PDF ManmadhaRaoDokument4 SeitenData PDF ManmadhaRaoBhavani Rao ReddiNoch keine Bewertungen
- St. Paul University Philippines Appendicitis PresentationDokument19 SeitenSt. Paul University Philippines Appendicitis PresentationAnaleah MalayaoNoch keine Bewertungen
- Acute Appendicitis by DR.S.HDokument24 SeitenAcute Appendicitis by DR.S.Hkevinharahap26Noch keine Bewertungen
- GIS-K-25 Acute Appendicitis Appendiceal Mass / AbscessDokument24 SeitenGIS-K-25 Acute Appendicitis Appendiceal Mass / AbscessYasmine Fitrina SiregarNoch keine Bewertungen
- Abdominal Distention inDokument45 SeitenAbdominal Distention inArif Rahman DmNoch keine Bewertungen
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryVon EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryNoch keine Bewertungen
- The Spleen - A Surgical Perspective: by Col. Abrar Hussain ZaidiDokument43 SeitenThe Spleen - A Surgical Perspective: by Col. Abrar Hussain Zaidiabrar_zaidiNoch keine Bewertungen
- Benign Breast Conditions 2Dokument38 SeitenBenign Breast Conditions 2abrar_zaidiNoch keine Bewertungen
- PeritonitisDokument34 SeitenPeritonitisabrar_zaidiNoch keine Bewertungen
- Groin Main (Dokument89 SeitenGroin Main (abrar_zaidi100% (2)
- How to Keep Your Heart HealthyDokument11 SeitenHow to Keep Your Heart HealthyLarissa RevillaNoch keine Bewertungen
- Gender-Dysphoric-Incongruene Persons, Guidelines JCEM 2017Dokument35 SeitenGender-Dysphoric-Incongruene Persons, Guidelines JCEM 2017Manel EMNoch keine Bewertungen
- Answer Sheet For Module 6: Pauline P. Dela CruzDokument4 SeitenAnswer Sheet For Module 6: Pauline P. Dela CruzPauline PascuaDNoch keine Bewertungen
- Sush Unity Haemotology-1700Dokument51 SeitenSush Unity Haemotology-1700Dr-Jahanzaib GondalNoch keine Bewertungen
- Trigeminal Neuralgia GuideDokument15 SeitenTrigeminal Neuralgia Guideandreas kevinNoch keine Bewertungen
- FUJIFILM's Antibacterial Technology - HYDRO AG'Dokument3 SeitenFUJIFILM's Antibacterial Technology - HYDRO AG'Colin BrownNoch keine Bewertungen
- Tall StatureDokument24 SeitenTall StaturedianmutiaNoch keine Bewertungen
- Drug StudyDokument17 SeitenDrug StudyTherese ArellanoNoch keine Bewertungen
- Fistulas Enterocutaneas MaingotDokument20 SeitenFistulas Enterocutaneas MaingotroyvillafrancaNoch keine Bewertungen
- Faktor PICODokument1 SeiteFaktor PICOAlldo SaodalaNoch keine Bewertungen
- Hipopresivos y Dolor Lumbar Cronico 2021Dokument9 SeitenHipopresivos y Dolor Lumbar Cronico 2021klgarivasNoch keine Bewertungen
- Manage Ophthalmia NeonatorumDokument2 SeitenManage Ophthalmia NeonatorumEjay BautistaNoch keine Bewertungen
- Health Apps - A ToolkitDokument3 SeitenHealth Apps - A ToolkitAlexandra WykeNoch keine Bewertungen
- Orthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Dokument13 SeitenOrthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Tomas Kurakovas100% (1)
- New Technologies Related To Public Health Electronic InformationDokument22 SeitenNew Technologies Related To Public Health Electronic InformationKhams TolentinoNoch keine Bewertungen
- SA Psych MAY 2016 FIn Final WebDokument82 SeitenSA Psych MAY 2016 FIn Final WebAKNTAI002Noch keine Bewertungen
- 2018 Conference AbstractsDokument155 Seiten2018 Conference AbstractsBanin AbadiNoch keine Bewertungen
- BiopharmaceuticsDokument52 SeitenBiopharmaceuticsDharma ShantiniNoch keine Bewertungen
- DR Jignesh ShahDokument6 SeitenDR Jignesh ShahBhavesh PatelNoch keine Bewertungen
- Medical Design BriefsDokument62 SeitenMedical Design Briefsneto512Noch keine Bewertungen
- A History of Prostate Cancer Cancer, Men and Medicine First Edition PDFDokument248 SeitenA History of Prostate Cancer Cancer, Men and Medicine First Edition PDFMarcela Osorio DugandNoch keine Bewertungen
- Living With CancerDokument400 SeitenLiving With CancerAnonymous FGqnrDuMNoch keine Bewertungen
- PALS Helpful Hints 2015 Guidelines Posted Nov 2016Dokument5 SeitenPALS Helpful Hints 2015 Guidelines Posted Nov 2016Mj Teate100% (1)
- Lincomycin: Drug Information: ALERT: US Boxed WarningDokument12 SeitenLincomycin: Drug Information: ALERT: US Boxed WarningsadiaNoch keine Bewertungen
- ImgDokument1 SeiteImgLIDIYA MOL P V100% (1)