Das könnte Ihnen auch gefallen
- HyperthyroidismDokument6 SeitenHyperthyroidismMalena Joy Ferraz VillanuevaNoch keine Bewertungen
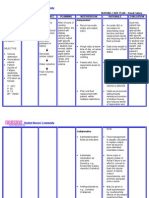
- Nursing Care Plan GoiterDokument3 SeitenNursing Care Plan Goiterdee_day_8100% (4)
- System Normal Abnormal Remarks Vital SignsDokument3 SeitenSystem Normal Abnormal Remarks Vital SignsJM RomiasNoch keine Bewertungen
- Colon Cancer Case Study - 64yo Male Diagnosed After Rectal BleedingDokument2 SeitenColon Cancer Case Study - 64yo Male Diagnosed After Rectal BleedingDragan Djordjevic100% (4)
- NCP-Esophageal Varices Pleural EffusionDokument6 SeitenNCP-Esophageal Varices Pleural Effusiontinatin98933% (3)
- Hypoparathyroidism: Low Calcium Caused by Parathyroid Gland IssuesDokument3 SeitenHypoparathyroidism: Low Calcium Caused by Parathyroid Gland IssuesSharmaine Grace Florig50% (2)
- Nursing Care Plans: Ineffective (Uteroplacental) Tissue PerfusionDokument2 SeitenNursing Care Plans: Ineffective (Uteroplacental) Tissue PerfusionVincent Paul SantosNoch keine Bewertungen
- Ov Ov OvDokument15 SeitenOv Ov OvHayyana Mae Taguba LadiaNoch keine Bewertungen
- Hemorrhoidectomy Case StudyDokument19 SeitenHemorrhoidectomy Case StudyJoyJoy Tabada CalunsagNoch keine Bewertungen
- Hyperthyroidism N C P BY BHERU LALDokument1 SeiteHyperthyroidism N C P BY BHERU LALBheru Lal100% (1)
- Risk For Compromised Human Dignity NCPDokument3 SeitenRisk For Compromised Human Dignity NCPMarife Lipana Reyes100% (3)
- Understanding Toxic Goiter and Its Nursing CareDokument22 SeitenUnderstanding Toxic Goiter and Its Nursing CareJohn Matley Caampued100% (2)
- Nursing Care Plan For Acyanotic Heart DiseaseDokument55 SeitenNursing Care Plan For Acyanotic Heart DiseaseDeepikaxena John79% (14)
- Thyroidectomy Nursing Care PlanDokument2 SeitenThyroidectomy Nursing Care PlanRnspeakcom100% (1)
- Case Study HemorrhoidsDokument4 SeitenCase Study HemorrhoidsTeanu Jose Gabrillo TamayoNoch keine Bewertungen
- Pathophysiology of Pain Stimuli and Nerve Fiber TransductionDokument1 SeitePathophysiology of Pain Stimuli and Nerve Fiber TransductionLorina Lynne Apelacio100% (2)
- 125.6 (Medicine) DISCHARGE PLANDokument1 Seite125.6 (Medicine) DISCHARGE PLANNadja Jamilah100% (1)
- Pedia With LeukemiaDokument14 SeitenPedia With LeukemiaAlynna ValbuenaNoch keine Bewertungen
- Massive AscitesDokument12 SeitenMassive Ascitesranitidin100% (1)
- Concept Mapping - Liver CirrhosisDokument3 SeitenConcept Mapping - Liver CirrhosisJoanna Mae MovidoNoch keine Bewertungen
- Pathophysiology of Cerebrovascular AccidentDokument2 SeitenPathophysiology of Cerebrovascular AccidentJohn Michael FernandezNoch keine Bewertungen
- Pathophysiology VolvulusDokument2 SeitenPathophysiology VolvulusHyacinth Bueser Bondad0% (2)
- Nutritional Management of StrokeDokument25 SeitenNutritional Management of StrokeChucky VergaraNoch keine Bewertungen
- Nursing Care Plan for Patient with LymphedemaDokument1 SeiteNursing Care Plan for Patient with Lymphedemayasira50% (2)
- Individual Case Study Acute GlomerulonephritisDokument26 SeitenIndividual Case Study Acute GlomerulonephritisBatrisyia HalimsNoch keine Bewertungen
- Preoperative and Post Liver Transplant Nursing Care PlanDokument5 SeitenPreoperative and Post Liver Transplant Nursing Care PlanOctoober67% (6)
- Pathophysiology of CholelithiasisDokument2 SeitenPathophysiology of CholelithiasisSherilNoch keine Bewertungen
- Nursing Care PlanDokument4 SeitenNursing Care PlanJoshua Pascasio100% (1)
- Esophageal Varices Causes Symptoms ManagementDokument2 SeitenEsophageal Varices Causes Symptoms ManagementSureen Regular100% (1)
- Anatomy and Physiology-Liver CirrhosisDokument2 SeitenAnatomy and Physiology-Liver CirrhosisHilmi Ramos100% (3)
- Dengue Fever Nursing Care PlansDokument6 SeitenDengue Fever Nursing Care PlansHikaru TakishimaNoch keine Bewertungen
- NCP GbsDokument2 SeitenNCP GbsJaylord VerazonNoch keine Bewertungen
- Nursing Diagnosis and Interventions for LeukemiaDokument6 SeitenNursing Diagnosis and Interventions for LeukemiaGeraldine Gallaron - Casipong67% (3)
- Proton Pump Inhibitor Suppresses Gastric AcidDokument1 SeiteProton Pump Inhibitor Suppresses Gastric AcidEngelbert CruzNoch keine Bewertungen
- Setting up a Balance Skeletal TractionDokument6 SeitenSetting up a Balance Skeletal Tractionandrea villanuevaNoch keine Bewertungen
- CholecystitisDokument60 SeitenCholecystitistammycristobalmd100% (15)
- Nursing Care Plan for Leukemia PatientDokument2 SeitenNursing Care Plan for Leukemia Patientخالد الغامديNoch keine Bewertungen
- HypoparathyroidismDokument6 SeitenHypoparathyroidismNader SmadiNoch keine Bewertungen
- Esophageal Stricture and ObstructionDokument11 SeitenEsophageal Stricture and ObstructionBibi Renu100% (6)
- NCP PancreatitisDokument2 SeitenNCP PancreatitisJeanelle GenerosoNoch keine Bewertungen
- Sexual history and STI examDokument2 SeitenSexual history and STI examLizaEllaga67% (3)
- PATHOPHYSIOLOGY Medicine Ward Client BasedDokument2 SeitenPATHOPHYSIOLOGY Medicine Ward Client BasedGem MarasiganNoch keine Bewertungen
- Case Study Pleural EffusionDokument4 SeitenCase Study Pleural EffusionKhristine Anne FabayNoch keine Bewertungen
- Caring for an Elderly Patient with DepressionDokument2 SeitenCaring for an Elderly Patient with DepressionSheryl Ann Barit PedinesNoch keine Bewertungen
- Medroxyprogesterone AcetateDokument3 SeitenMedroxyprogesterone Acetateapi-3797941Noch keine Bewertungen
- Nursing DiagnosisvfsdsDokument2 SeitenNursing DiagnosisvfsdsPrincess Gutierrez Rosita100% (1)
- Precipitous Labor/Delivery or Unplanned/Out-of-Hospital DeliveryDokument7 SeitenPrecipitous Labor/Delivery or Unplanned/Out-of-Hospital DeliveryLei Ortega100% (1)
- Class 2 Lesson PlanDokument16 SeitenClass 2 Lesson PlanArjun Neupane100% (1)
- Case Study ON Hodgkin LymphomaDokument8 SeitenCase Study ON Hodgkin LymphomaMeena KoushalNoch keine Bewertungen
- Pathophysiology Sickle Cell AnemiaDokument1 SeitePathophysiology Sickle Cell AnemiaTine GuibaoNoch keine Bewertungen
- Pathophysiology of StrokeDokument3 SeitenPathophysiology of StrokeAqeel Al-Mahdaly0% (1)
- Tranexamic Acid Nursing ResponsibilitiesDokument1 SeiteTranexamic Acid Nursing Responsibilitiesjanmalexx100% (4)
- Amniotic Fluid EmbolismDokument30 SeitenAmniotic Fluid EmbolismDonmer Ibañez Juan100% (1)
- NCP - TBDokument2 SeitenNCP - TBPahw BaluisNoch keine Bewertungen
- Post-Throidectomy Nursing Care PlanDokument2 SeitenPost-Throidectomy Nursing Care PlanCyrus De AsisNoch keine Bewertungen
- Nursing Care Plan Renal FailureDokument2 SeitenNursing Care Plan Renal FailureMark Jason Rabadan100% (1)
- Activity 2 MetabsDokument10 SeitenActivity 2 MetabsCalvin Keith YadaoNoch keine Bewertungen
- Community Health Final Exam ReviewDokument4 SeitenCommunity Health Final Exam ReviewkcharmaigneNoch keine Bewertungen
- Concept MapDokument9 SeitenConcept MapAllene PaderangaNoch keine Bewertungen
- Case Presentation On CKD/AKIDokument29 SeitenCase Presentation On CKD/AKIsalma.nasr003Noch keine Bewertungen
- The Places You'll Go PDFDokument12 SeitenThe Places You'll Go PDFLyra Lorca71% (7)
- Head TraumaDokument66 SeitenHead Traumamara514089% (9)
- How Successful People ThinkDokument9 SeitenHow Successful People ThinkLyra LorcaNoch keine Bewertungen
- As a Man Thinketh - How Thoughts Shape Character and CircumstancesDokument21 SeitenAs a Man Thinketh - How Thoughts Shape Character and CircumstancesAndrez LopezNoch keine Bewertungen
- Anatomy and Physiology of The HeartDokument22 SeitenAnatomy and Physiology of The HeartCarimaGhalie100% (2)
- Communicable DiseasesDokument19 SeitenCommunicable Diseasesriamanabat100% (5)
- Common Drug Stems Cheat SheetDokument2 SeitenCommon Drug Stems Cheat SheetCharis Mae DimaculanganNoch keine Bewertungen
- Stephen CoveyDokument18 SeitenStephen CoveyAbhijith Shetty100% (2)
- Cranial Nerves FormDokument2 SeitenCranial Nerves FormbarbaraNoch keine Bewertungen
- How To Maximise Your Life Brian Houston 31 DayDokument48 SeitenHow To Maximise Your Life Brian Houston 31 DayMarcelo MendiondoNoch keine Bewertungen
- CD NotesDokument9 SeitenCD NotesOmar Christian TuazonNoch keine Bewertungen
- Myocardial InfarctionDokument3 SeitenMyocardial InfarctionLyra LorcaNoch keine Bewertungen
- Laws Affecting Nursing Practice RA's: Heherson AlvarezDokument2 SeitenLaws Affecting Nursing Practice RA's: Heherson AlvarezGeevee Naganag VentulaNoch keine Bewertungen
- 20 Amino AcidsDokument1 Seite20 Amino AcidsLyra LorcaNoch keine Bewertungen
- 17 Indisputable Laws of TeamworkDokument18 Seiten17 Indisputable Laws of TeamworkFred Raphael IlomoNoch keine Bewertungen
- Cur Dev ReportDokument2 SeitenCur Dev ReportLyra LorcaNoch keine Bewertungen
- Consent FormDokument1 SeiteConsent FormLyra LorcaNoch keine Bewertungen
- Nurse OpportunitiesDokument36 SeitenNurse OpportunitiesLyra LorcaNoch keine Bewertungen
- OR FormDokument1 SeiteOR FormLyra LorcaNoch keine Bewertungen
- OR FormDokument1 SeiteOR FormLyra LorcaNoch keine Bewertungen
- PathophysiologyDokument1 SeitePathophysiologyLyra LorcaNoch keine Bewertungen
- Wounded Healers DirectionDokument2 SeitenWounded Healers DirectionLyra LorcaNoch keine Bewertungen
- Schistosomiasis Fact SheetDokument1 SeiteSchistosomiasis Fact SheetLyra LorcaNoch keine Bewertungen
- SchistosomiasisDokument6 SeitenSchistosomiasisLyra LorcaNoch keine Bewertungen
- Medical Care: "Microbiology, Epidemiology, Clinical Manifestations, and Diagnosis of Leptospirosis"Dokument5 SeitenMedical Care: "Microbiology, Epidemiology, Clinical Manifestations, and Diagnosis of Leptospirosis"Lyra LorcaNoch keine Bewertungen
- Photo Therapy and Bili LightDokument5 SeitenPhoto Therapy and Bili LightLyra LorcaNoch keine Bewertungen
- TuberculosisDokument5 SeitenTuberculosisLyra LorcaNoch keine Bewertungen
- Abruptio Placenta - OutputDokument2 SeitenAbruptio Placenta - OutputLyra LorcaNoch keine Bewertungen
- Placenta Previa - OutputDokument2 SeitenPlacenta Previa - OutputLyra LorcaNoch keine Bewertungen
- TuberculosisDokument5 SeitenTuberculosisLyra LorcaNoch keine Bewertungen
- Letter of Invitation For The ReactorDokument2 SeitenLetter of Invitation For The ReactorImmah PinedaNoch keine Bewertungen
- FST556 - Dietary Fibre ObeDokument37 SeitenFST556 - Dietary Fibre Obeinshirahizham100% (1)
- Philippines UPR JointReport 3rdcycleDokument15 SeitenPhilippines UPR JointReport 3rdcycleJojana Christine GeneralNoch keine Bewertungen
- No Hipertensi Harga (RP) PaketDokument2 SeitenNo Hipertensi Harga (RP) PaketVania Azalia HariyantoNoch keine Bewertungen
- Categories and Sources of Data: 1. Direct Method: There Are Three Methods Under The Direct MethodDokument3 SeitenCategories and Sources of Data: 1. Direct Method: There Are Three Methods Under The Direct MethodMaharshi UpadhyayNoch keine Bewertungen
- Facilitating Behavior ChangeDokument9 SeitenFacilitating Behavior ChangeJohn Carlo PerezNoch keine Bewertungen
- Speech by SakiDokument2 SeitenSpeech by Sakiapi-516439363Noch keine Bewertungen
- Action Planning For ToRs of CMT - XLSX CompleteDokument1 SeiteAction Planning For ToRs of CMT - XLSX CompleteOSCAR RUHWEZANoch keine Bewertungen
- (Events) Interview With Julia EvettsDokument6 Seiten(Events) Interview With Julia Evettsneelam100% (1)
- Anatomy Physiology and Disease An Interactive Journey For Health Professions 2nd Edition Colbert Test BankDokument32 SeitenAnatomy Physiology and Disease An Interactive Journey For Health Professions 2nd Edition Colbert Test BankAliciaMcintoshaeiop100% (13)
- Anesthesia Techniques for Supratentorial Tumor SurgeryDokument35 SeitenAnesthesia Techniques for Supratentorial Tumor SurgeryChalis NovrizaNoch keine Bewertungen
- UNDER FIVES CLINICDokument4 SeitenUNDER FIVES CLINICJyoti SidhuNoch keine Bewertungen
- q1 Grade 7 Pe DLL Week 1Dokument13 Seitenq1 Grade 7 Pe DLL Week 1MildremMae Olaer AbingNoch keine Bewertungen
- OPTIMIZE GROUND OPERATIONSDokument3 SeitenOPTIMIZE GROUND OPERATIONSAshwin Leonard100% (3)
- Wound Care ChecklistDokument5 SeitenWound Care Checklistacademic purposes100% (1)
- Augmentative and Alternative Communication Practice Guide PDFDokument73 SeitenAugmentative and Alternative Communication Practice Guide PDFCarolina LilloNoch keine Bewertungen
- Catatan Hortatory Exposition - 2ndDokument4 SeitenCatatan Hortatory Exposition - 2ndDennis Stwn100% (1)
- Detection of Brain HemorrhageDokument8 SeitenDetection of Brain HemorrhageIJRASETPublicationsNoch keine Bewertungen
- Thu Thao PDFDokument10 SeitenThu Thao PDFDienNoch keine Bewertungen
- Central Mindanao University College of Nursing NGT Insertion ProcedureDokument3 SeitenCentral Mindanao University College of Nursing NGT Insertion ProcedureDARWIN JAY SANG-ANNoch keine Bewertungen
- Assessment of Learning (First Quarter) in Physical Education 1 Most Learned Competencies Learning Competency CodeDokument3 SeitenAssessment of Learning (First Quarter) in Physical Education 1 Most Learned Competencies Learning Competency CodeRames Ely GJNoch keine Bewertungen
- Basic Counselor's Attending Skills & ResponsesDokument20 SeitenBasic Counselor's Attending Skills & ResponsesDARRO6 FOINoch keine Bewertungen
- ThunderBay Event RevisedDokument1 SeiteThunderBay Event RevisedLyane ZygmuntNoch keine Bewertungen
- ENANTIODROMIADokument2 SeitenENANTIODROMIAJohn SmithNoch keine Bewertungen
- 3710Dokument9 Seiten3710Asad KhanNoch keine Bewertungen
- Surgical Methods Accelerate Tooth MovementDokument7 SeitenSurgical Methods Accelerate Tooth MovementSneha JoshiNoch keine Bewertungen
- Enterprise 9000X (E9X) : Instruction For UseDokument68 SeitenEnterprise 9000X (E9X) : Instruction For UsePiotr KaczorNoch keine Bewertungen
- The Salesman Analysis by Tanmay TandonDokument2 SeitenThe Salesman Analysis by Tanmay TandonTanmay TandonNoch keine Bewertungen
- DepEd Padre Garcia District Webinar on Transitioning to the New NormalDokument10 SeitenDepEd Padre Garcia District Webinar on Transitioning to the New NormalARLENE MARASIGANNoch keine Bewertungen
- 4 - Weiss2 - NASEM Overview of Trace Minerals and Vitamin RequirementsDokument8 Seiten4 - Weiss2 - NASEM Overview of Trace Minerals and Vitamin RequirementsbboybmasterNoch keine Bewertungen