Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- MedicationsDokument3 SeitenMedicationsapi-237061134Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Study Group Term 2Dokument1 SeiteStudy Group Term 2api-237061134Noch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoulder VindicateDokument1 SeiteShoulder Vindicateapi-237061134Noch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- GH OrthopaedicsDokument3 SeitenGH Orthopaedicsapi-237256827Noch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Fibroids PresentationDokument6 SeitenFibroids Presentationapi-237061134Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Lex NervesDokument1 SeiteLex Nervesapi-237061134Noch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Fibroids PresentationDokument6 SeitenFibroids Presentationapi-237061134Noch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elbow VindicateDokument1 SeiteElbow Vindicateapi-237061134Noch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- LSPDokument8 SeitenLSPapi-237061134Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Op Cca Formative ExamDokument1 SeiteOp Cca Formative Examapi-237061134Noch keine Bewertungen
- CSP VindicateDokument1 SeiteCSP Vindicateapi-237061134Noch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Op Cca Formative ExamDokument1 SeiteOp Cca Formative Examapi-237061134Noch keine Bewertungen
- TSP VindicateDokument1 SeiteTSP Vindicateapi-237061134Noch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Cervical Radiculopathy Nice GuidelinesDokument3 SeitenCervical Radiculopathy Nice Guidelinesapi-237061134Noch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Decompression SurgeryDokument9 SeitenDecompression Surgeryapi-238049665Noch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Op Cca Formative ExamDokument1 SeiteOp Cca Formative Examapi-237061134Noch keine Bewertungen
- Cspine Nice GuidelinesDokument5 SeitenCspine Nice Guidelinesapi-237061134Noch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Good Sources of Carb Protein FatDokument2 SeitenGood Sources of Carb Protein Fatapi-237061134Noch keine Bewertungen
- SIJ VindicateDokument1 SeiteSIJ Vindicateapi-237061134Noch keine Bewertungen
- Neck Pain - Non-Specific NiceDokument3 SeitenNeck Pain - Non-Specific Niceapi-237061134Noch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- LumbarvindicateDokument1 SeiteLumbarvindicateapi-237061134Noch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
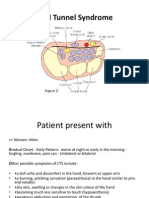
- Carpal Tunnel Syndrome Power Point PresentationDokument6 SeitenCarpal Tunnel Syndrome Power Point Presentationapi-237061134Noch keine Bewertungen
- Lami Disc ForaDokument9 SeitenLami Disc Foraapi-237061134Noch keine Bewertungen
- Pubic SymphysisDokument1 SeitePubic Symphysisapi-237061134Noch keine Bewertungen
- Knee VindicateDokument2 SeitenKnee Vindicateapi-237061134Noch keine Bewertungen
- Foot-Vindicate-Study GroupDokument1 SeiteFoot-Vindicate-Study Groupapi-237061134Noch keine Bewertungen
- Hip VindicateDokument1 SeiteHip Vindicateapi-237061134Noch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Miqueias Leone Learning ContractDokument3 SeitenMiqueias Leone Learning Contractapi-237061134Noch keine Bewertungen
- Hallux ValgusDokument2 SeitenHallux Valgusapi-237061134Noch keine Bewertungen
- Paediatric Dosage of Some Drugs-1Dokument45 SeitenPaediatric Dosage of Some Drugs-1JaneNoch keine Bewertungen
- Role Play Discharge PlanningDokument3 SeitenRole Play Discharge PlanningChoirunnisa Putri100% (1)
- Jurnal Zinc HiperbilirubinemiaDokument5 SeitenJurnal Zinc HiperbilirubinemiaAbdurrohman IzzuddinNoch keine Bewertungen
- Understanding Triage: Three Sorts and Cases: Frank BraioDokument23 SeitenUnderstanding Triage: Three Sorts and Cases: Frank BraioAdelina RotaruNoch keine Bewertungen
- OB PACU Severe PreeclampsiaDokument65 SeitenOB PACU Severe Preeclampsiasurbakti_christineNoch keine Bewertungen
- Full FragranceDokument47 SeitenFull FragranceVladimir Ilic0% (1)
- Vaccination CertificateDokument14 SeitenVaccination Certificatemayorga fireNoch keine Bewertungen
- Introduction To Clinical Psychology Notes 1Dokument83 SeitenIntroduction To Clinical Psychology Notes 1Paulo Miguel GernaleNoch keine Bewertungen
- Feed MixDokument4 SeitenFeed MixTony1248Noch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Instructions - For - Use ValtocoDokument2 SeitenInstructions - For - Use Valtocofreebass08Noch keine Bewertungen
- FemaraDokument2 SeitenFemaraMyraIntisarNoch keine Bewertungen
- Ayurveda MD Panchakarma Academics DissertationDokument38 SeitenAyurveda MD Panchakarma Academics DissertationManish KubawatNoch keine Bewertungen
- The Bruininks-Oseretsky Test of Motor Proficiency - Second Edition (BOT-2)Dokument2 SeitenThe Bruininks-Oseretsky Test of Motor Proficiency - Second Edition (BOT-2)Mikey PanupongNoch keine Bewertungen
- List of Licensed Private and Public Hospital 2011Dokument7 SeitenList of Licensed Private and Public Hospital 2011TJ NgNoch keine Bewertungen
- Renal QuizDokument2 SeitenRenal Quizgladz25Noch keine Bewertungen
- Category 3: Mammography (Digital) : 1260023072PL - Alpha - XLSX 1 of 15Dokument15 SeitenCategory 3: Mammography (Digital) : 1260023072PL - Alpha - XLSX 1 of 15Berkant Orçun ÇangalNoch keine Bewertungen
- Maastricht Interview For ChildrenDokument14 SeitenMaastricht Interview For ChildrenlillouanaNoch keine Bewertungen
- AlexionDokument2 SeitenAlexionLiz HartNoch keine Bewertungen
- Ross Rabindranath Mission Issue-2Dokument24 SeitenRoss Rabindranath Mission Issue-2RanenDasguptaNoch keine Bewertungen
- Human Kinetics Web Resources PDFDokument4 SeitenHuman Kinetics Web Resources PDFyou waggaNoch keine Bewertungen
- Tanda - Tanda VitalDokument4 SeitenTanda - Tanda VitalImelda ChristinaNoch keine Bewertungen
- Yati Soenarto - RACP AucklandDokument34 SeitenYati Soenarto - RACP AucklandIntan HartandyNoch keine Bewertungen
- Delta Sigma Theta Sorority, Inc. Jacksonville Alumnae ChapterDokument7 SeitenDelta Sigma Theta Sorority, Inc. Jacksonville Alumnae ChaptermortensenkNoch keine Bewertungen
- Pta 1010 Observation Hours PaperDokument3 SeitenPta 1010 Observation Hours Paperapi-269101384Noch keine Bewertungen
- The Bridge, June 26, 2014Dokument28 SeitenThe Bridge, June 26, 2014The BridgeNoch keine Bewertungen
- Pulmonary Science: Local Learning For Global SuccessDokument2 SeitenPulmonary Science: Local Learning For Global SuccessedwaNoch keine Bewertungen
- Biocompactability Testing of Medical DevicesDokument5 SeitenBiocompactability Testing of Medical DevicesSathesh Kumar Annamalai100% (1)
- Classical Homoeopathy Book FourDokument99 SeitenClassical Homoeopathy Book FourYaniv Algrably100% (1)
- 4 6001055797780414555 PDFDokument245 Seiten4 6001055797780414555 PDFAtomNoch keine Bewertungen
- 123Dokument10 Seiten123Aryan SanezNoch keine Bewertungen
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (24)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)