Das könnte Ihnen auch gefallen
- TAHBSO ReportDokument4 SeitenTAHBSO ReportsachiiMeNoch keine Bewertungen
- Pre Op Nursing CareDokument4 SeitenPre Op Nursing CareAyaBasilio100% (1)
- 6 Hysterectomy/TAHBSO Nursing Care Plans: Low Self-EsteemDokument5 Seiten6 Hysterectomy/TAHBSO Nursing Care Plans: Low Self-Esteemonlyone_unik0% (1)
- Nursing Care Plan for Acute Pain ManagementDokument3 SeitenNursing Care Plan for Acute Pain ManagementSheene Lysethea Sioteco AguilosNoch keine Bewertungen
- NCP Risk For InfectionDokument6 SeitenNCP Risk For InfectionCazze SunioNoch keine Bewertungen
- Ex LapDokument42 SeitenEx LapOmar Khalif Amad PendatunNoch keine Bewertungen
- NCP TahbsoDokument18 SeitenNCP TahbsoKe EjieNoch keine Bewertungen
- NCPs For ParotidectomyDokument8 SeitenNCPs For ParotidectomyAcohCChao100% (1)
- Thyroidectomy Nursing Care PlanDokument2 SeitenThyroidectomy Nursing Care PlanRnspeakcom100% (1)
- NCP Patient 3 Cervical CADokument8 SeitenNCP Patient 3 Cervical CAFatima LabaoNoch keine Bewertungen
- NCP Modified Radical MastectomyDokument5 SeitenNCP Modified Radical MastectomyIvan Jules P. PALMARESNoch keine Bewertungen
- TAHBSO Concept MapDokument1 SeiteTAHBSO Concept MapSherika Mariz Moreno GuarinNoch keine Bewertungen
- NCP BkaDokument4 SeitenNCP BkaKeeshia CesnerosNoch keine Bewertungen
- NCP - OsteosarcomaDokument5 SeitenNCP - OsteosarcomaNelson Lacsamana100% (1)
- Managing Post-Surgical Abdominal PainDokument2 SeitenManaging Post-Surgical Abdominal PainKaren ValdezNoch keine Bewertungen
- NCP IntraDokument1 SeiteNCP IntraCharlene Valerie Alviola0% (1)
- NCP: FracturesDokument21 SeitenNCP: FracturesJavie100% (1)
- Discharge PlanDokument2 SeitenDischarge PlanRoxanne_Buenaf_5285Noch keine Bewertungen
- Spinal Cord Injury NCPDokument2 SeitenSpinal Cord Injury NCPEmmanuelRodriguez100% (1)
- NCP HemothoraxDokument3 SeitenNCP HemothoraxMichael John F. NatividadNoch keine Bewertungen
- Pathophysiology of Uterine CancerDokument1 SeitePathophysiology of Uterine CancerCharlotte Cordero0% (1)
- Ov Ov OvDokument15 SeitenOv Ov OvHayyana Mae Taguba LadiaNoch keine Bewertungen
- Duties of Circulating NurseDokument2 SeitenDuties of Circulating NurseAchie_Abie_5891100% (1)
- (NCPS) Impaired Physical Mobility 2Dokument2 Seiten(NCPS) Impaired Physical Mobility 2roren100% (1)
- Erceflora Antidiarrheal ClassDokument1 SeiteErceflora Antidiarrheal ClassfLOR_ZIANE_MAENoch keine Bewertungen
- NCP - Fluid Volume DeficitDokument2 SeitenNCP - Fluid Volume DeficitPatrice LimNoch keine Bewertungen
- Exploratory Laparotomy Procedure ExplainedDokument5 SeitenExploratory Laparotomy Procedure ExplainedChristopher Timothy100% (1)
- Operating Room WriteDokument2 SeitenOperating Room WritemodiNoch keine Bewertungen
- SunStar News Doctors May Lose Their Licenses Over Surgery ScandalDokument4 SeitenSunStar News Doctors May Lose Their Licenses Over Surgery Scandalseigelystic100% (12)
- Roles and Responsibilities of Head, Med and Staff NurseDokument3 SeitenRoles and Responsibilities of Head, Med and Staff NurseTrish 0019Noch keine Bewertungen
- Risk For InfectionDokument3 SeitenRisk For Infectionprickybiik100% (1)
- NCP Leptospirosis - NewDokument5 SeitenNCP Leptospirosis - Newglaiza_requintoNoch keine Bewertungen
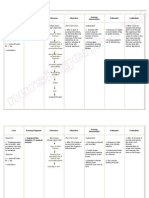
- Cues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale EvaluationDokument4 SeitenCues Nursing Diagnosis Scientific Reason Objective Nursing Intervention Rationale Evaluationjomsportg0% (1)
- Nursing Crib Com NURSING CARE PLAN Spontaneous AbortionDokument2 SeitenNursing Crib Com NURSING CARE PLAN Spontaneous AbortionJustin PasaronNoch keine Bewertungen
- 00.00 Reference Care Plan Tonsillectomy and Adnoidectomy Post OpDokument5 Seiten00.00 Reference Care Plan Tonsillectomy and Adnoidectomy Post OpMarya KemmieNoch keine Bewertungen
- NCP Infection NewDokument3 SeitenNCP Infection NewXerxes DejitoNoch keine Bewertungen
- Cancer Nursing Care Plan (NCP) - Risk For InfectionDokument2 SeitenCancer Nursing Care Plan (NCP) - Risk For InfectionAngie MandeoyaNoch keine Bewertungen
- Discharge Plan Medication and Health TeachingsDokument6 SeitenDischarge Plan Medication and Health Teachingsqueenieann100% (1)
- 4 NCP - Acute Pain FinalDokument3 Seiten4 NCP - Acute Pain FinalElisha Gine AndalesNoch keine Bewertungen
- Breast Cancer PathophysiologyDokument3 SeitenBreast Cancer PathophysiologyJM Andrade100% (3)
- NCP Ineffective Breathing GunshotDokument3 SeitenNCP Ineffective Breathing GunshotMikko Enoc100% (1)
- Impaired urinary elimination diagnosis and interventionsDokument4 SeitenImpaired urinary elimination diagnosis and interventionsEji AsouNoch keine Bewertungen
- NCP AppendicitisDokument1 SeiteNCP AppendicitisNiña AngNoch keine Bewertungen
- Anatomy and Physiology Related To Multiple Myelom1Dokument15 SeitenAnatomy and Physiology Related To Multiple Myelom1Diane Kate Tobias Magno100% (1)
- GENERIC NAME: Co-Amoxiclav (Amoxicillin & Clavulanic Acid) BRAND NAMES: Natravox, AddexDokument4 SeitenGENERIC NAME: Co-Amoxiclav (Amoxicillin & Clavulanic Acid) BRAND NAMES: Natravox, AddexDRANoch keine Bewertungen
- Mastectomy Case Study ObjectivesDokument2 SeitenMastectomy Case Study ObjectivesJClaudz Pilapil100% (1)
- Nursing Care for Surgical Incision HealingDokument2 SeitenNursing Care for Surgical Incision HealingJrose CuerpoNoch keine Bewertungen
- Nursing Care Plan for Breast CancerDokument2 SeitenNursing Care Plan for Breast CancerMaina BarmanNoch keine Bewertungen
- Set 5Dokument18 SeitenSet 5Dick Morgan FerrerNoch keine Bewertungen
- CAD Discharge PlanDokument2 SeitenCAD Discharge PlanmamiudamNoch keine Bewertungen
- NCP PainDokument2 SeitenNCP PainKarizza Reyes Mamaradlo100% (1)
- Nursing Care Plan Impaire Physical MobilityDokument2 SeitenNursing Care Plan Impaire Physical Mobilityderic90% (10)
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDokument4 SeitenTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNoch keine Bewertungen
- Sources of Stress As Per: Student's Academic Performance Effects of StressDokument14 SeitenSources of Stress As Per: Student's Academic Performance Effects of StressMacrina PatocNoch keine Bewertungen
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeDokument2 SeitenTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Pre-OperativeMiar QuestNoch keine Bewertungen
- Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Post-OperativeDokument2 SeitenTotal Abdominal Hysterectomy Bilateral Salpingo Oophorectomy (Tahbso) Nursing Responsibilities Rationale Post-OperativeMiar QuestNoch keine Bewertungen
- AssignmentDokument6 SeitenAssignmentEduard GarchitorenaNoch keine Bewertungen
- Endoscopic Procedure (Nursing Responsibilities)Dokument4 SeitenEndoscopic Procedure (Nursing Responsibilities)YessaminNoch keine Bewertungen
- Periop Power PointDokument97 SeitenPeriop Power PointAldrine Albor Anyayahan INoch keine Bewertungen
- Care of Surgical Patients - 1Dokument14 SeitenCare of Surgical Patients - 1mr.moutkalanNoch keine Bewertungen
- Drug StudyDokument2 SeitenDrug StudysugarmontejoNoch keine Bewertungen
- Pathophysiology of Acute Renal FailureDokument2 SeitenPathophysiology of Acute Renal Failuresugarmontejo67% (3)
- One Love and Kapayapaan LyricsDokument1 SeiteOne Love and Kapayapaan LyricssugarmontejoNoch keine Bewertungen
- Physical Examination and Review of SystemsDokument1 SeitePhysical Examination and Review of SystemssugarmontejoNoch keine Bewertungen
- Nursing Health AssessmentDokument4 SeitenNursing Health AssessmentsugarmontejoNoch keine Bewertungen
- Nursing Assessment IIDokument4 SeitenNursing Assessment IIsugarmontejoNoch keine Bewertungen
- Nursing Care Plan: Cues Objectives Interventions Rationale EvaluationDokument1 SeiteNursing Care Plan: Cues Objectives Interventions Rationale EvaluationsugarmontejoNoch keine Bewertungen
- Demographic Data & Health HistoryDokument1 SeiteDemographic Data & Health HistorysugarmontejoNoch keine Bewertungen
- Clinical Teaching PLANDokument2 SeitenClinical Teaching PLANsugarmontejoNoch keine Bewertungen
- Date Medication Dosage Route Frequency Remarks: Summary of MedicationsDokument8 SeitenDate Medication Dosage Route Frequency Remarks: Summary of MedicationssugarmontejoNoch keine Bewertungen
- Drug Study DengueDokument3 SeitenDrug Study DengueiamELHIZANoch keine Bewertungen
- Lima Modular Revision Hip SystemDokument32 SeitenLima Modular Revision Hip SystemjsdanielinNoch keine Bewertungen
- Pain Myocardial: Review Treatment of in InfarctionDokument5 SeitenPain Myocardial: Review Treatment of in InfarctionAlifah ChoNoch keine Bewertungen
- Music and MoodDokument5 SeitenMusic and MoodNatalia TríasNoch keine Bewertungen
- Maths On The Move' - Effectiveness of Physically-Active Lessons For Learning Maths and Increasing Physical Activity in Primary School StudentsDokument22 SeitenMaths On The Move' - Effectiveness of Physically-Active Lessons For Learning Maths and Increasing Physical Activity in Primary School Studentsiisu-cmse libraryNoch keine Bewertungen
- Compartment SyndromeDokument29 SeitenCompartment SyndromeFazmial UjirNoch keine Bewertungen
- Ecg InterpretationDokument3 SeitenEcg Interpretationman0billi0% (1)
- Obat SpesialisDokument16 SeitenObat SpesialisLAILATUL AFIYAHNoch keine Bewertungen
- 1 - General Indications and Contraindications - 2019 - Lumbar Interbody FusionsDokument12 Seiten1 - General Indications and Contraindications - 2019 - Lumbar Interbody FusionsSergiu MalinNoch keine Bewertungen
- Firstaid ModuleDokument143 SeitenFirstaid Moduleretni wulandariNoch keine Bewertungen
- 37 Percent Formaldehyde Aqueous Solution Mixture of Hcho Ch3oh and H2o Sds p6224Dokument12 Seiten37 Percent Formaldehyde Aqueous Solution Mixture of Hcho Ch3oh and H2o Sds p6224Juan Esteban LopezNoch keine Bewertungen
- Artifacts in Hematology by Dr. Bakul DalalDokument11 SeitenArtifacts in Hematology by Dr. Bakul DalalDr MayurNoch keine Bewertungen
- Nexthealth - Semantic Web Sparks Evolution of Health 2.0 - A Road Map To Consumer-Centric HealthcareDokument7 SeitenNexthealth - Semantic Web Sparks Evolution of Health 2.0 - A Road Map To Consumer-Centric HealthcareMaarten den Braber100% (43)
- Youtsey Kristen Cover LetterDokument1 SeiteYoutsey Kristen Cover Letterapi-457850399Noch keine Bewertungen
- Tacoma-Pierce County Health Department - E-Cigarette E-Mails April 2011 Part 1Dokument292 SeitenTacoma-Pierce County Health Department - E-Cigarette E-Mails April 2011 Part 1American Vaping AssociationNoch keine Bewertungen
- Clinical Manifestations, Diagnosis, and Surgery of Inferior Oblique Muscle EctopiaDokument5 SeitenClinical Manifestations, Diagnosis, and Surgery of Inferior Oblique Muscle EctopiaMuhammad Imam NoorNoch keine Bewertungen
- 3 Wives One Husband 2Dokument508 Seiten3 Wives One Husband 2relebohilelehasa2Noch keine Bewertungen
- Subcutaneous MycosesDokument23 SeitenSubcutaneous Mycosessarguss14100% (1)
- Surgical Treatment For BREAST CANCERDokument5 SeitenSurgical Treatment For BREAST CANCERJericho James TopacioNoch keine Bewertungen
- Narcotics and Antimigraine Agents (AE, Drug-Drug Interactions)Dokument5 SeitenNarcotics and Antimigraine Agents (AE, Drug-Drug Interactions)ShiraishiNoch keine Bewertungen
- Closing The Gap 2012Dokument127 SeitenClosing The Gap 2012ABC News OnlineNoch keine Bewertungen
- Concept Map Draft ExampleDokument2 SeitenConcept Map Draft ExamplemeliNoch keine Bewertungen
- 2023 - Clinical Scales For Headache Disorders (Pınar Yalınay Dikmen Aynur Özge)Dokument318 Seiten2023 - Clinical Scales For Headache Disorders (Pınar Yalınay Dikmen Aynur Özge)César Escobar100% (1)
- Introduction To Dental Anatomy: DR - Yad Raouf BDS, Efb, MrcsedDokument27 SeitenIntroduction To Dental Anatomy: DR - Yad Raouf BDS, Efb, MrcsedRabarNoch keine Bewertungen
- AYR Patient Experience PresentationDokument29 SeitenAYR Patient Experience Presentationaustin_tx6Noch keine Bewertungen
- Vivid I and Vivid Q Cardiovascular Ultrasound: SectorDokument4 SeitenVivid I and Vivid Q Cardiovascular Ultrasound: SectorShaikh Emran HossainNoch keine Bewertungen
- Ateneo de Zamboanga University Nursing Skills Output (NSO) Week BiopsyDokument4 SeitenAteneo de Zamboanga University Nursing Skills Output (NSO) Week BiopsyHaifi HunNoch keine Bewertungen
- CelecoxibDokument2 SeitenCelecoxibLaromac RolandNoch keine Bewertungen
- Development of Push-Pull Osmotic Pump Tablets For A SlightlyDokument4 SeitenDevelopment of Push-Pull Osmotic Pump Tablets For A SlightlyphamuyenthuNoch keine Bewertungen
- Pharmacoeconomics - Part IIIDokument29 SeitenPharmacoeconomics - Part IIISima JabbariNoch keine Bewertungen