Das könnte Ihnen auch gefallen
- Infection Control Nurse: Passbooks Study GuideVon EverandInfection Control Nurse: Passbooks Study GuideNoch keine Bewertungen
- Infection Control CommitteeDokument7 SeitenInfection Control Committeefarha naazNoch keine Bewertungen
- Handbook for Cssd Technicians: Understanding the Basics - Second EditionVon EverandHandbook for Cssd Technicians: Understanding the Basics - Second EditionNoch keine Bewertungen
- Hospital DocumentsDokument17 SeitenHospital DocumentsRaviraj PisheNoch keine Bewertungen
- Sri Lakshmi Medical Centre Hospital Infection Control ManualDokument59 SeitenSri Lakshmi Medical Centre Hospital Infection Control Manualdhir.ankurNoch keine Bewertungen
- Infection Control ManualDokument51 SeitenInfection Control Manuallimiya varghese100% (1)
- Hic ManualDokument260 SeitenHic ManualVamshi Narean Naidu100% (3)
- Infection Control in ICUDokument7 SeitenInfection Control in ICUzenagit123456Noch keine Bewertungen
- Patient SafetyDokument22 SeitenPatient SafetyRensy Sabi100% (1)
- HIC Manual (2015-2016) PDFDokument161 SeitenHIC Manual (2015-2016) PDFparth_desi100% (1)
- Infection Prevention and Control Policies and Guidelines For Health Care ServicesDokument324 SeitenInfection Prevention and Control Policies and Guidelines For Health Care ServicesAlejandro Caballero ChumillasNoch keine Bewertungen
- Role of Nursing in Infection ControlDokument54 SeitenRole of Nursing in Infection Controltummalapalli venkateswara rao75% (4)
- Hospital SopsDokument12 SeitenHospital Sopspratimaz80% (5)
- Hospital Organization and Its ServicesDokument40 SeitenHospital Organization and Its ServicesNidhiNoch keine Bewertungen
- Ward SopDokument45 SeitenWard SopRhod Bernaldez Esta100% (7)
- Infection Control Manual 1Dokument54 SeitenInfection Control Manual 1Botanic Hair Oil100% (1)
- Hospital Infection Control Guidelines-2Dokument103 SeitenHospital Infection Control Guidelines-2Sri KishoreNoch keine Bewertungen
- 2019 HICC Manual CMCDokument170 Seiten2019 HICC Manual CMCmujeeb86% (14)
- KSA hospital infection control manualDokument205 SeitenKSA hospital infection control manualSalah ElbadawyNoch keine Bewertungen
- Prevention of Hospital Acquired InfectionDokument39 SeitenPrevention of Hospital Acquired Infectionbtalera80% (5)
- Infection Control Assessment ToolDokument30 SeitenInfection Control Assessment ToolPMNoch keine Bewertungen
- Infection Control Audit Tool - July 2009Dokument50 SeitenInfection Control Audit Tool - July 2009rachael_duff100% (6)
- 1 Paper EmergencyDepartmentPatientProcessFlowDokument6 Seiten1 Paper EmergencyDepartmentPatientProcessFlowandika fahruroziNoch keine Bewertungen
- Nabh and JciDokument12 SeitenNabh and JciPooja Kabbur50% (2)
- Committee and Meetings (Infection Control)Dokument3 SeitenCommittee and Meetings (Infection Control)Lua CJ100% (5)
- Manual of Infection Control ProceduresDokument365 SeitenManual of Infection Control Proceduressgupta_532847100% (4)
- Compliance rate study of bio-medical waste segregationDokument50 SeitenCompliance rate study of bio-medical waste segregationAman Dheer Kapoor100% (2)
- ICN Nurse Job ResponsibilitiesDokument2 SeitenICN Nurse Job ResponsibilitiesBirupakshya RoutNoch keine Bewertungen
- Infection Control NurseDokument1 SeiteInfection Control NurseAhmed Mostafa100% (2)
- Concepts of Infection ControlDokument53 SeitenConcepts of Infection ControlPak Pandir0% (1)
- Quality Improvement in A HospitalDokument30 SeitenQuality Improvement in A HospitalSunita Abraham100% (2)
- Nabh Entry LevelDokument64 SeitenNabh Entry LevelRenuka MuruganNoch keine Bewertungen
- Poorvi CSSD PROJECTDokument45 SeitenPoorvi CSSD PROJECTPiaNoch keine Bewertungen
- New Assessment Tool For HospitalsDokument60 SeitenNew Assessment Tool For HospitalssaguliteNoch keine Bewertungen
- In Patient Wardrs ChecklistDokument4 SeitenIn Patient Wardrs ChecklistDnyanesh AitalwadNoch keine Bewertungen
- NABH Assessor Checklist for Entry Level HospitalDokument64 SeitenNABH Assessor Checklist for Entry Level Hospitalkaushik karmakar100% (3)
- Infection Control ManualDokument51 SeitenInfection Control ManualIka C Purnomo100% (2)
- Emergency Department PolicyDokument18 SeitenEmergency Department PolicySt. Mary's HospitalNoch keine Bewertungen
- Fire Safety NABHDokument10 SeitenFire Safety NABHDrNitin Sippy100% (3)
- Hospital PharmacyDokument10 SeitenHospital PharmacyWassema ShaikNoch keine Bewertungen
- HOSPITAL INVENTORY CONTROL'S IMPORTANCEDokument64 SeitenHOSPITAL INVENTORY CONTROL'S IMPORTANCEvaibhav_ng3363100% (2)
- Ic ManualDokument416 SeitenIc ManualEvangel PaduaNoch keine Bewertungen
- Whole Hospital Policy 011111Dokument43 SeitenWhole Hospital Policy 011111ummuawisy100% (7)
- Operation Theatre GuidelinesDokument5 SeitenOperation Theatre Guidelines21jouhar86% (7)
- Ot Utilization Project 642Dokument69 SeitenOt Utilization Project 642Amit Pahwa100% (3)
- MRD ProtocolDokument27 SeitenMRD ProtocolVarun Marar67% (3)
- Bio Medical Waste ManagementDokument5 SeitenBio Medical Waste Managementanantarao75% (4)
- Infection Control: Dr.T.V.Rao MD Professor of MicrobiologyDokument41 SeitenInfection Control: Dr.T.V.Rao MD Professor of Microbiologytummalapalli venkateswara rao100% (1)
- Hospital Infection Control Program StandardsDokument14 SeitenHospital Infection Control Program StandardsLorelie Asis100% (1)
- Checklist For NABH StandardsDokument9 SeitenChecklist For NABH StandardsNanak BarikNoch keine Bewertungen
- Hospital Accreditation Program: National Accreditation Board For Hospitals & Healthcare Providers (Nabh)Dokument21 SeitenHospital Accreditation Program: National Accreditation Board For Hospitals & Healthcare Providers (Nabh)rrvlsolutionsNoch keine Bewertungen
- Infection Control in CSSDDokument44 SeitenInfection Control in CSSDAzira Afzan100% (1)
- MRD ProjectDokument23 SeitenMRD Projectsamgill66916Noch keine Bewertungen
- Antibiotics Audit ChecklistDokument1 SeiteAntibiotics Audit ChecklistPrabhat Kumar100% (1)
- SP Hic Manual PDFDokument76 SeitenSP Hic Manual PDFANTO MATHINoch keine Bewertungen
- File571 PDFDokument65 SeitenFile571 PDFSri KishoreNoch keine Bewertungen
- Hospital Infection Control Committee GuideDokument5 SeitenHospital Infection Control Committee GuideShehnaz SheikhNoch keine Bewertungen
- p.1-2 - Standards in Infection Control For Healthcare FacilitiesDokument19 Seitenp.1-2 - Standards in Infection Control For Healthcare FacilitiestiredandsleepyNoch keine Bewertungen
- Infection Control Policy5967286291Dokument41 SeitenInfection Control Policy5967286291Shyam PrasadNoch keine Bewertungen
- HOSPITAL INFECTION PREVENTION AND CONTROL GUIDELINESDokument65 SeitenHOSPITAL INFECTION PREVENTION AND CONTROL GUIDELINESRazaCreciaLastrillaMenesesNoch keine Bewertungen
- MusculoskeletalDokument146 SeitenMusculoskeletalcfqbcm5swbNoch keine Bewertungen
- Guide To Case Presentation-1Dokument36 SeitenGuide To Case Presentation-1Amanda Rodriguez TejedaNoch keine Bewertungen
- ABG QuizDokument13 SeitenABG QuizSSNoch keine Bewertungen
- Anbio IFU English 1 JusteradDokument3 SeitenAnbio IFU English 1 JusteradVasilij PupkinNoch keine Bewertungen
- Elective 102 Module 4 Activities:: Test Your Nursing KnowledgeDokument5 SeitenElective 102 Module 4 Activities:: Test Your Nursing KnowledgeEsmareldah Henry SirueNoch keine Bewertungen
- Ophthalmologic Manifestations Revealing Posterior Reversible Encephalopathy Syndrome: A Case ReportDokument5 SeitenOphthalmologic Manifestations Revealing Posterior Reversible Encephalopathy Syndrome: A Case ReportIJAR JOURNALNoch keine Bewertungen
- Caregiving 9 - Maintain A Clean and Hygienic EnvironmentDokument24 SeitenCaregiving 9 - Maintain A Clean and Hygienic EnvironmentKATHRYN ALFONSONoch keine Bewertungen
- Encefalitis LimbicaDokument11 SeitenEncefalitis LimbicaRandy UlloaNoch keine Bewertungen
- Human Health and Diseases Imp QuestionsDokument21 SeitenHuman Health and Diseases Imp QuestionsMadhumathi SSNoch keine Bewertungen
- Spinal Anatomy 101Dokument25 SeitenSpinal Anatomy 101Monleau céliaNoch keine Bewertungen
- Clase 03 - Inglés IiDokument26 SeitenClase 03 - Inglés IiIngenieria y Construccion SherkensNoch keine Bewertungen
- 01-SHWM-Introduction (Compatibility Mode) PDFDokument30 Seiten01-SHWM-Introduction (Compatibility Mode) PDFhungarianNoch keine Bewertungen
- Intervention Action Plan-StressDokument14 SeitenIntervention Action Plan-Stressapi-545050593Noch keine Bewertungen
- Pathophysiology - Rheumatoid ArthritisDokument1 SeitePathophysiology - Rheumatoid ArthritisAngel FiloteoNoch keine Bewertungen
- Gouty Arthritis: Tarlac State University College of Science Nursing DepartmentDokument22 SeitenGouty Arthritis: Tarlac State University College of Science Nursing DepartmentKrisianne Mae Lorenzo FranciscoNoch keine Bewertungen
- 6.2 Health Declaration Form - EmployeeDokument1 Seite6.2 Health Declaration Form - EmployeeyyNoch keine Bewertungen
- Pyrexia of Unknown Origin 3Dokument27 SeitenPyrexia of Unknown Origin 3Ausu OfficialNoch keine Bewertungen
- Encefalitis ViralDokument8 SeitenEncefalitis ViralRubenNoch keine Bewertungen
- DLC PracticalDokument6 SeitenDLC PracticalAngoruz Gohain BaruahNoch keine Bewertungen
- Applied Anatomy of Spinal CordDokument34 SeitenApplied Anatomy of Spinal CordSuhana PathanNoch keine Bewertungen
- Immunizations Health TeachingDokument9 SeitenImmunizations Health TeachingClaudine Jo B. TalabocNoch keine Bewertungen
- Ingles Caderno de Provas e Chave de Respostas - Edital 07-2023Dokument8 SeitenIngles Caderno de Provas e Chave de Respostas - Edital 07-2023Eduarda HelenaNoch keine Bewertungen
- NCM 112 - Med SurgDokument7 SeitenNCM 112 - Med SurgKierzteen Brianna TaromaNoch keine Bewertungen
- Bio-Psycho-Social Formulation and Differential Diagnosis: Psychiatric Assessment With Helen M. Farrell, M.DDokument12 SeitenBio-Psycho-Social Formulation and Differential Diagnosis: Psychiatric Assessment With Helen M. Farrell, M.DJ.C. GarzaNoch keine Bewertungen
- Chapter 128 - Thyroid and Adrenal Disorders: Episode OverviewDokument15 SeitenChapter 128 - Thyroid and Adrenal Disorders: Episode OverviewIkenna EzeiloNoch keine Bewertungen
- Weekly Influenza Surveillance Update 2020-2021 From The Rhode Island Department of Health.Dokument29 SeitenWeekly Influenza Surveillance Update 2020-2021 From The Rhode Island Department of Health.Frank MaradiagaNoch keine Bewertungen
- CAPC Key Messages Re - COVID-19-Center To Advance Palliative Care PDFDokument1 SeiteCAPC Key Messages Re - COVID-19-Center To Advance Palliative Care PDFSergio Rafael Medina VillelaNoch keine Bewertungen
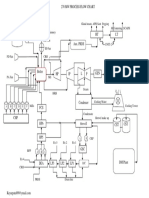
- Power Plant Process Flow Chart PDFDokument1 SeitePower Plant Process Flow Chart PDFFikriHidayatullahNoch keine Bewertungen
- Houseman Exam Paper 1Dokument10 SeitenHouseman Exam Paper 1baby raneeNoch keine Bewertungen
- Blumea BalsamiferaDokument4 SeitenBlumea BalsamiferaNeill DepalacNoch keine Bewertungen
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (402)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingVon EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingBewertung: 5 von 5 Sternen5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (13)
- The Happiness Trap: How to Stop Struggling and Start LivingVon EverandThe Happiness Trap: How to Stop Struggling and Start LivingBewertung: 4 von 5 Sternen4/5 (1)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNoch keine Bewertungen
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 5 von 5 Sternen5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNoch keine Bewertungen
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesVon EverandThe Ultimate Guide To Memory Improvement TechniquesBewertung: 5 von 5 Sternen5/5 (34)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsVon EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNoch keine Bewertungen
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingVon EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingBewertung: 3.5 von 5 Sternen3.5/5 (31)
- Techniques Exercises And Tricks For Memory ImprovementVon EverandTechniques Exercises And Tricks For Memory ImprovementBewertung: 4.5 von 5 Sternen4.5/5 (40)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisVon EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisBewertung: 5 von 5 Sternen5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (253)
- Secure Love: Create a Relationship That Lasts a LifetimeVon EverandSecure Love: Create a Relationship That Lasts a LifetimeBewertung: 5 von 5 Sternen5/5 (17)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (327)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (44)