Das könnte Ihnen auch gefallen
- Clement Li - Aging and Emerging Technologies PaperDokument16 SeitenClement Li - Aging and Emerging Technologies Paperapi-251641757Noch keine Bewertungen
- Drblashewicz ReferenceDokument2 SeitenDrblashewicz Referenceapi-251641757Noch keine Bewertungen
- Clement Li - Autism Spectrum Disorder Critical Research PaperDokument13 SeitenClement Li - Autism Spectrum Disorder Critical Research Paperapi-251641757Noch keine Bewertungen
- Clement Li - Legal BriefDokument6 SeitenClement Li - Legal Briefapi-251641757Noch keine Bewertungen
- Overview V 2Dokument4 SeitenOverview V 2api-251641757Noch keine Bewertungen
- App Framework V 3Dokument7 SeitenApp Framework V 3api-251641757Noch keine Bewertungen
- Indesign AshxDokument21 SeitenIndesign Ashxapi-251641757Noch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- History of Special Education in the PhilippinesDokument8 SeitenHistory of Special Education in the PhilippinesAngelica Marin100% (4)
- UCSP Reviewer LawDokument6 SeitenUCSP Reviewer LawEJ RaveloNoch keine Bewertungen
- Triple CDokument2 SeitenTriple CBethany Keily100% (1)
- Assess functional abilities with 17-item scaleDokument5 SeitenAssess functional abilities with 17-item scaleJose Paul RaderNoch keine Bewertungen
- SPED Action Plan of SchoolsDokument2 SeitenSPED Action Plan of SchoolsMarjorie IdianNoch keine Bewertungen
- Samarthanam ProfileDokument12 SeitenSamarthanam ProfilemyndsetsNoch keine Bewertungen
- GiftAbled Holistic Approach 2022Dokument13 SeitenGiftAbled Holistic Approach 2022vinnshineNoch keine Bewertungen
- Binder 3-13141Dokument93 SeitenBinder 3-13141Anubhav JainNoch keine Bewertungen
- MCA Second Year 4 Sem Exam FormDokument67 SeitenMCA Second Year 4 Sem Exam Formvidya patilNoch keine Bewertungen
- Learning Disabilities Association of Ontario Ldao 2Dokument4 SeitenLearning Disabilities Association of Ontario Ldao 2api-366074669Noch keine Bewertungen
- WORKBOOK SUBJECT 7 CHCAGE004 Implement Interventions With Older People at Risk CHCAGE003 Co OrdinatDokument181 SeitenWORKBOOK SUBJECT 7 CHCAGE004 Implement Interventions With Older People at Risk CHCAGE003 Co Ordinatklm klm100% (1)
- BG HealthAndSafetyDokument60 SeitenBG HealthAndSafetyVasile NodisNoch keine Bewertungen
- Expounding The Rehabilitation Service For Acquired Visual Impairment Contingent On Assistive Technology AcceptanceDokument6 SeitenExpounding The Rehabilitation Service For Acquired Visual Impairment Contingent On Assistive Technology AcceptanceNicolas MendezNoch keine Bewertungen
- Classroom Activity CHCDIS003Dokument4 SeitenClassroom Activity CHCDIS003Sonam GurungNoch keine Bewertungen
- Vending Machine LetterDokument1 SeiteVending Machine LetterTarah TaylorNoch keine Bewertungen
- Haverfordwest Tennis Club Membership Form 2018-2019Dokument2 SeitenHaverfordwest Tennis Club Membership Form 2018-2019Gareth RobinsonNoch keine Bewertungen
- I Am SamDokument4 SeitenI Am SamEmJay BalansagNoch keine Bewertungen
- UT Dallas Syllabus For Psy4327.501 06f Taught by Edward Davis (Ecd022000)Dokument5 SeitenUT Dallas Syllabus For Psy4327.501 06f Taught by Edward Davis (Ecd022000)UT Dallas Provost's Technology GroupNoch keine Bewertungen
- Philippians 4 13 - PPT DEFENSEDokument17 SeitenPhilippians 4 13 - PPT DEFENSESherwina Marie del RosarioNoch keine Bewertungen
- Case 10 Shutter IslandDokument3 SeitenCase 10 Shutter IslandAnkith ReddyNoch keine Bewertungen
- Abnormal Psychology: Clinical Perspectives On Psychological Disorders PDF - Descargar, LeerDokument10 SeitenAbnormal Psychology: Clinical Perspectives On Psychological Disorders PDF - Descargar, Leerroven desuNoch keine Bewertungen
- (B) Evaluate The Characteristics, Types and Measures of Schizophrenia and Psychotic Disorders, Including A Discussion of Case StudiesDokument1 Seite(B) Evaluate The Characteristics, Types and Measures of Schizophrenia and Psychotic Disorders, Including A Discussion of Case StudiesHenry Nguyen PhamNoch keine Bewertungen
- 177 211110 1659555955 Paper 1 06112021 Pam Northern Chapter Webinar ms1184pptxDokument65 Seiten177 211110 1659555955 Paper 1 06112021 Pam Northern Chapter Webinar ms1184pptxFong Wei JunNoch keine Bewertungen
- Williams and Mavin 2012Dokument21 SeitenWilliams and Mavin 2012fionakumaricampbell6631Noch keine Bewertungen
- CAMPBELL, F.K. Exploring Internalized AbleismDokument18 SeitenCAMPBELL, F.K. Exploring Internalized AbleismBruna DomingosNoch keine Bewertungen
- Job Application FormDokument8 SeitenJob Application FormCreative SuccessNoch keine Bewertungen
- Summary of Anxiety Disorders (DSM-5)Dokument6 SeitenSummary of Anxiety Disorders (DSM-5)Villamorchard100% (3)
- Abi LympicsDokument24 SeitenAbi LympicsSMNoch keine Bewertungen
- Communication Skills For Children With Severe Learning DifficultiesDokument10 SeitenCommunication Skills For Children With Severe Learning DifficultiesMay Grace E. BalbinNoch keine Bewertungen
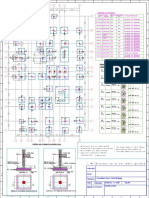
- Column and Footing Plan (22!02!2022) APDokument1 SeiteColumn and Footing Plan (22!02!2022) APRanjit BarmanNoch keine Bewertungen