Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Instant Download Ebook PDF Abrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition PDF ScribdDokument38 SeitenInstant Download Ebook PDF Abrams Clinical Drug Therapy Rationales For Nursing Practice 11th Edition PDF Scribdkimberly.davis644100% (41)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Cervical MyelopathyDokument18 SeitenCervical MyelopathyRangga InktaenNdoek'sNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- 363 Conf 2 Prep Sheet Portfolio TeamsDokument1 Seite363 Conf 2 Prep Sheet Portfolio Teamsapi-254154139Noch keine Bewertungen
- Thesis ReferencesDokument5 SeitenThesis Referencesapi-254154139Noch keine Bewertungen
- SP Proposalv1 s14Dokument6 SeitenSP Proposalv1 s14api-254154139Noch keine Bewertungen
- 363 SPR 2014 Marc SyllabusDokument7 Seiten363 SPR 2014 Marc Syllabusapi-254154139Noch keine Bewertungen
- SP WN Complete s14Dokument20 SeitenSP WN Complete s14api-254154139Noch keine Bewertungen
- SP Coverletter s141Dokument4 SeitenSP Coverletter s141api-254154139Noch keine Bewertungen
- SP Thesispresentation s14Dokument36 SeitenSP Thesispresentation s14api-254154139Noch keine Bewertungen
- KushaDokument4 SeitenKushaapi-254088508Noch keine Bewertungen
- Proposal Final Version1Dokument13 SeitenProposal Final Version1api-254154139Noch keine Bewertungen
- Gastro Esophageal Reflux Disease: (Case Study)Dokument7 SeitenGastro Esophageal Reflux Disease: (Case Study)nj02Noch keine Bewertungen
- Optic Disk Drusen in ChildrenDokument14 SeitenOptic Disk Drusen in ChildrenPriscila VerduzcoNoch keine Bewertungen
- Inflamasi Akut Dan Kronik. 1Dokument40 SeitenInflamasi Akut Dan Kronik. 1shintaandiNoch keine Bewertungen
- Solid TumoursDokument48 SeitenSolid TumoursViswanadh BNoch keine Bewertungen
- 1 . - FDA EscitalopramDokument34 Seiten1 . - FDA EscitalopramMary FallNoch keine Bewertungen
- Advanced Electrolysis TechniquesDokument2 SeitenAdvanced Electrolysis Techniquesandres mesaNoch keine Bewertungen
- Pancreatitis Case StudyDokument11 SeitenPancreatitis Case Studysunny kumarNoch keine Bewertungen
- 29 Paramedic Quizzes, Questions, Answers & TriviaDokument1 Seite29 Paramedic Quizzes, Questions, Answers & TriviaCris AtNoch keine Bewertungen
- Oral Exostoses: An Assessment of Two Hundred Years of Research Les Exostoses Orales: Bilan de Deux Siècles de RecherchesDokument22 SeitenOral Exostoses: An Assessment of Two Hundred Years of Research Les Exostoses Orales: Bilan de Deux Siècles de RecherchesYusuf DiansyahNoch keine Bewertungen
- Chapter 21Dokument37 SeitenChapter 21Ivan Olo SarumpaetNoch keine Bewertungen
- A Visit To The Doctor - EnfermeriaDokument4 SeitenA Visit To The Doctor - EnfermeriaSILVIA MARIELA LLAMOCA LIMACHENoch keine Bewertungen
- Musculoskeletal Bulletin: Research Informing PracticeDokument2 SeitenMusculoskeletal Bulletin: Research Informing PracticeElena DolcanNoch keine Bewertungen
- Anabolic SteroidsDokument5 SeitenAnabolic SteroidsGideon MurathaNoch keine Bewertungen
- Dr. Nazim Mughal: Ms Ortho, DNB Ortho FNB Spine SurgeryDokument90 SeitenDr. Nazim Mughal: Ms Ortho, DNB Ortho FNB Spine Surgerynazim mughalNoch keine Bewertungen
- How To Help Prevent Eating Disorders?Dokument7 SeitenHow To Help Prevent Eating Disorders?Sebastián ValenciaNoch keine Bewertungen
- Core 1 - Health Priorities in Australia - Notes (Neilab Osman)Dokument50 SeitenCore 1 - Health Priorities in Australia - Notes (Neilab Osman)chelsea nightingaleNoch keine Bewertungen
- Manual Muscle Test (MMT) : Ajith C Student of Department of Physio Kmch-CoptDokument80 SeitenManual Muscle Test (MMT) : Ajith C Student of Department of Physio Kmch-Coptayesha solNoch keine Bewertungen
- Iub 9999 0Dokument13 SeitenIub 9999 0Simona VisanNoch keine Bewertungen
- Nursing Care Plan (NCP) For Acute Lymphocytic LeukemiaDokument4 SeitenNursing Care Plan (NCP) For Acute Lymphocytic LeukemiaromelynNoch keine Bewertungen
- Graphites 01 PDFDokument3 SeitenGraphites 01 PDFASLAMNoch keine Bewertungen
- Directors Duties Indg417Dokument12 SeitenDirectors Duties Indg417Muhammad RidwanNoch keine Bewertungen
- Full Medical Alert ListDokument2 SeitenFull Medical Alert ListCarlosDanielNoch keine Bewertungen
- 32 Okuthe Fao Isavet and VlcsDokument15 Seiten32 Okuthe Fao Isavet and VlcsObo KeroNoch keine Bewertungen
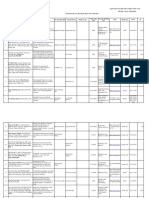
- Danh Sach Bai Bao Quoc Te 2020 794Dokument14 SeitenDanh Sach Bai Bao Quoc Te 2020 794Master DrNoch keine Bewertungen
- COVID-19 Nepal: Preparedness and Response Plan (NPRPDokument56 SeitenCOVID-19 Nepal: Preparedness and Response Plan (NPRPKrishnaNoch keine Bewertungen
- 9447-Article Text-33080-1-10-20160306Dokument10 Seiten9447-Article Text-33080-1-10-20160306Nagib MuhammadNoch keine Bewertungen
- 12 Steps of AA in 40 CharactersDokument11 Seiten12 Steps of AA in 40 Charactersmike9diaz-689513Noch keine Bewertungen
- Esophagus - Anatomy and Development - GI Motility OnlineDokument21 SeitenEsophagus - Anatomy and Development - GI Motility OnlineMaria Fernanda VargasNoch keine Bewertungen