Das könnte Ihnen auch gefallen
- Employee Details FormDokument2 SeitenEmployee Details FormVilhas DesaiNoch keine Bewertungen
- Regular Employee Details FormDokument4 SeitenRegular Employee Details FormRajesh BabuNoch keine Bewertungen
- No Dues FormDokument2 SeitenNo Dues FormSourabh Sharma100% (1)
- Address ProofDokument1 SeiteAddress Proofsrikar dasaradhiNoch keine Bewertungen
- Personal Information: Employee Data Base FormDokument3 SeitenPersonal Information: Employee Data Base FormMohit GuptaNoch keine Bewertungen
- Employment Background Verification FormDokument7 SeitenEmployment Background Verification FormAnchit Aggarwal0% (2)
- Employee Verification FormDokument7 SeitenEmployee Verification FormEric RowlandNoch keine Bewertungen
- Form 13Dokument3 SeitenForm 13ArunNoch keine Bewertungen
- Employee Joining FormDokument2 SeitenEmployee Joining FormSwapnashree Das100% (1)
- Candidate Information Sheet-V5Dokument4 SeitenCandidate Information Sheet-V5sriraman sriNoch keine Bewertungen
- Name Change Correction FormDokument1 SeiteName Change Correction Formombir saini100% (2)
- Appointment Letter Cimarex Energy CoDokument2 SeitenAppointment Letter Cimarex Energy CoSaugat KarNoch keine Bewertungen
- Form - Exit InterviewDokument6 SeitenForm - Exit Interviewjohn sladeNoch keine Bewertungen
- Employee Background Verification FormDokument3 SeitenEmployee Background Verification FormAnupam0103Noch keine Bewertungen
- Employee Joining FormDokument2 SeitenEmployee Joining FormSK SORIFUL ISLAMNoch keine Bewertungen
- Background Verification FormDokument10 SeitenBackground Verification Formashish10mcaNoch keine Bewertungen
- PETRONAS Declaration FormDokument2 SeitenPETRONAS Declaration FormAidzawati Abd Azih0% (1)
- Background Verification Form - Seaton India IT Private LimitedDokument5 SeitenBackground Verification Form - Seaton India IT Private LimitedMaheshKandguleNoch keine Bewertungen
- Candidate Declaration FormDokument8 SeitenCandidate Declaration FormDon RajuNoch keine Bewertungen
- Affinity Employee Joining Form - Nupur LuthraDokument3 SeitenAffinity Employee Joining Form - Nupur LuthravandanaNoch keine Bewertungen
- Pre-Joining Doc Checklist & BGC Form V-6Dokument11 SeitenPre-Joining Doc Checklist & BGC Form V-6salman.azhar uddinNoch keine Bewertungen
- Employee Joining FormDokument35 SeitenEmployee Joining FormNikita NikiNoch keine Bewertungen
- Appointment LetterDokument3 SeitenAppointment LetterSwapnashree DasNoch keine Bewertungen
- Employee Joining Form LivosoDokument2 SeitenEmployee Joining Form LivosoKali RathNoch keine Bewertungen
- Employee's Salary FormDokument2 SeitenEmployee's Salary FormConnie AlisasisNoch keine Bewertungen
- SBI Car Loan Application FormDokument6 SeitenSBI Car Loan Application FormKarthik Gunasekaran100% (2)
- BGV Form CfirstDokument10 SeitenBGV Form Cfirstsunil singhNoch keine Bewertungen
- Vijayapura: Background Verification FormDokument8 SeitenVijayapura: Background Verification FormUday GowdaNoch keine Bewertungen
- Employment Application Form - Campus - V02 - Effective 11th May 2015Dokument8 SeitenEmployment Application Form - Campus - V02 - Effective 11th May 2015jai prakashNoch keine Bewertungen
- Letter of Authorization (Genpact)Dokument3 SeitenLetter of Authorization (Genpact)Jennelyn SulitNoch keine Bewertungen
- Employee Information FormDokument3 SeitenEmployee Information Formjamil AhmadNoch keine Bewertungen
- Candidate Information Sheet-V6Dokument4 SeitenCandidate Information Sheet-V6ishNoch keine Bewertungen
- No Dues Checklist: AdministrationDokument2 SeitenNo Dues Checklist: AdministrationpraneethNoch keine Bewertungen
- Kura Job Application FormDokument3 SeitenKura Job Application Formpaul machariaNoch keine Bewertungen
- Schengen Visa - Covering LetterDokument1 SeiteSchengen Visa - Covering LettersamNoch keine Bewertungen
- Increment Letter FormatDokument2 SeitenIncrement Letter FormatPavankumar KarnamNoch keine Bewertungen
- Wipro Company Application FormDokument4 SeitenWipro Company Application FormSmital Solanki100% (1)
- Joining LetterDokument1 SeiteJoining LetterAbu Zafor0% (1)
- Full and Final SettlementDokument1 SeiteFull and Final Settlementbhupendrasharma00Noch keine Bewertungen
- Offer of Employment and Employment ContractDokument3 SeitenOffer of Employment and Employment ContracttrainershipsolutionsNoch keine Bewertungen
- Application For Employment (Executive Appointment)Dokument5 SeitenApplication For Employment (Executive Appointment)jammushaNoch keine Bewertungen
- Labour Contract - Agreement FormDokument4 SeitenLabour Contract - Agreement FormManoj YadavNoch keine Bewertungen
- Background Verification FormDokument5 SeitenBackground Verification FormMANO RAJNoch keine Bewertungen
- Expense Reimbursement FormDokument5 SeitenExpense Reimbursement FormGilang Anggit PambudiNoch keine Bewertungen
- PF Nomination FormDokument3 SeitenPF Nomination FormNarendra GaurNoch keine Bewertungen
- Job Application Form at URSB: Please Fill in All The Information (Where Applicable) 1. Personal InformationDokument4 SeitenJob Application Form at URSB: Please Fill in All The Information (Where Applicable) 1. Personal InformationsdsadsadNoch keine Bewertungen
- Anubhuti Foundation Membership Form: Full Name: Guardian's NameDokument2 SeitenAnubhuti Foundation Membership Form: Full Name: Guardian's NameSUBHAM HAZRA100% (1)
- EMPLYEE JOINING FORM-2003 FormatDokument4 SeitenEMPLYEE JOINING FORM-2003 FormatBhavesh VijayvargiyaNoch keine Bewertungen
- Employee Information FormDokument1 SeiteEmployee Information FormxixaNoch keine Bewertungen
- Offer Letter For JobDokument1 SeiteOffer Letter For JobJahid HasanNoch keine Bewertungen
- Bosch Application FormDokument9 SeitenBosch Application FormEr Balaji Patra100% (1)
- Guntupalli Akhil - Offer LetterDokument8 SeitenGuntupalli Akhil - Offer LetterGuntupalli akhilNoch keine Bewertungen
- Iso CertificateDokument2 SeitenIso CertificateSupriyaNoch keine Bewertungen
- Employee Self Verification FormDokument6 SeitenEmployee Self Verification Formdharsan321Noch keine Bewertungen
- ?KKS"K.KK I K: 4-Tue DH FRFFK Fnu Eghuk O"Kz 5 - Osokfgd Fookfgr@ Izkflfkfr Vfookfgr Fo/KokDokument4 Seiten?KKS"K.KK I K: 4-Tue DH FRFFK Fnu Eghuk O"Kz 5 - Osokfgd Fookfgr@ Izkflfkfr Vfookfgr Fo/KokHarsha VardhanNoch keine Bewertungen
- ESIC SPECIMEN - Form-1 Declaration FormDokument2 SeitenESIC SPECIMEN - Form-1 Declaration FormnimishshrivastavNoch keine Bewertungen
- Ilovepdf MergedDokument6 SeitenIlovepdf MergedHarsha VardhanNoch keine Bewertungen
- Form 1Dokument4 SeitenForm 1singhkaur20232023Noch keine Bewertungen
- Form-1 ESI Declaration FormDokument26 SeitenForm-1 ESI Declaration FormKalyaan ThotteNoch keine Bewertungen
- Daniel Pandey: E-Mail AddressDokument3 SeitenDaniel Pandey: E-Mail AddressDaniel PandeyNoch keine Bewertungen
- Canovan - Populism For Political Theorists¿Dokument13 SeitenCanovan - Populism For Political Theorists¿sebatorres7Noch keine Bewertungen
- Launch Your Organization With WebGISDokument17 SeitenLaunch Your Organization With WebGISkelembagaan telitiNoch keine Bewertungen
- C - WEST SIDE STORY (Mambo) - Guitare 2Dokument1 SeiteC - WEST SIDE STORY (Mambo) - Guitare 2Giuseppe CrimiNoch keine Bewertungen
- Veneranda Dini Anggraeni 201071058 Grammer Mini TestDokument18 SeitenVeneranda Dini Anggraeni 201071058 Grammer Mini TestAyu DaratistaNoch keine Bewertungen
- Libanan, Et Al. v. GordonDokument33 SeitenLibanan, Et Al. v. GordonAlvin ComilaNoch keine Bewertungen
- Read MeDokument21 SeitenRead MeSyafaruddin BachrisyahNoch keine Bewertungen
- Wood Magazine 253 05.2018 PDFDokument92 SeitenWood Magazine 253 05.2018 PDFJd Diaz83% (6)
- 2022 Post Report - FinalDokument11 Seiten2022 Post Report - FinalAise TrigoNoch keine Bewertungen
- Delhi To AhmedabadDokument2 SeitenDelhi To Ahmedabad02 Raihan Ahmedi 2997Noch keine Bewertungen
- English 6: Making A On An InformedDokument30 SeitenEnglish 6: Making A On An InformedEDNALYN TANNoch keine Bewertungen
- Was Poll Tax The Most Important Reason For Margaret Thatchers Downfall?Dokument5 SeitenWas Poll Tax The Most Important Reason For Margaret Thatchers Downfall?wendyfoxNoch keine Bewertungen
- The Role of Black Consciousness in The Experience of Being Black in South-Mphikeleni Mattew MnguniDokument136 SeitenThe Role of Black Consciousness in The Experience of Being Black in South-Mphikeleni Mattew MngunimylesNoch keine Bewertungen
- Riph - Prelim ReviewerDokument12 SeitenRiph - Prelim ReviewerNikoru100% (3)
- In Organic We TrustDokument5 SeitenIn Organic We Trustapi-511313050Noch keine Bewertungen
- HR 2977 - Space Preservation Act of 2001Dokument6 SeitenHR 2977 - Space Preservation Act of 2001Georg ElserNoch keine Bewertungen
- Testimonies and PioneersDokument4 SeitenTestimonies and Pioneerswally ziembickiNoch keine Bewertungen
- India International SchoolDokument15 SeitenIndia International Schoolazimmuhammed673790Noch keine Bewertungen
- Strategic Management CompleteDokument20 SeitenStrategic Management Completeأبو ليلىNoch keine Bewertungen
- Substituted by The Income-Tax (6th Amendment) Rule, 2019, W.E.F. 5-11-2019Dokument5 SeitenSubstituted by The Income-Tax (6th Amendment) Rule, 2019, W.E.F. 5-11-2019dpfsopfopsfhopNoch keine Bewertungen
- Office of The Divisional Forest Officer, Durgapur DivisionDokument30 SeitenOffice of The Divisional Forest Officer, Durgapur Divisionrchowdhury_10Noch keine Bewertungen
- NPD and VMSDokument4 SeitenNPD and VMSK V S MadaanNoch keine Bewertungen
- People vs. Nadera, JR.: 490 Supreme Court Reports AnnotatedDokument11 SeitenPeople vs. Nadera, JR.: 490 Supreme Court Reports AnnotatedFatzie MendozaNoch keine Bewertungen
- LUL S1062 - Temporary Works - Issue A4Dokument29 SeitenLUL S1062 - Temporary Works - Issue A4HNoch keine Bewertungen
- JustdiggitDokument21 SeitenJustdiggityecith sanguinoNoch keine Bewertungen
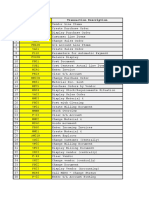
- # Transaction Code Transaction DescriptionDokument6 Seiten# Transaction Code Transaction DescriptionVivek Shashikant SonawaneNoch keine Bewertungen
- PAIN POINTS - Can Be Conscious (Actual Demand) or Unconscious (Latent Demand) That CanDokument8 SeitenPAIN POINTS - Can Be Conscious (Actual Demand) or Unconscious (Latent Demand) That CanGeorge PaulNoch keine Bewertungen
- Tes Sharing Agreement 1Dokument2 SeitenTes Sharing Agreement 1Chesca UrietaNoch keine Bewertungen
- Andres Felipe Mendez Vargas: The Elves and The ShoemakerDokument1 SeiteAndres Felipe Mendez Vargas: The Elves and The ShoemakerAndres MendezNoch keine Bewertungen
- Atip Bin Ali V Josephine Doris Nunis & AnorDokument7 SeitenAtip Bin Ali V Josephine Doris Nunis & Anorahmad fawwaz100% (1)
- Jayant CVDokument2 SeitenJayant CVjayanttiwariNoch keine Bewertungen