Das könnte Ihnen auch gefallen
- Iloilo Doctors' College College of Nursing West Avenue, Molo, Iloilo City Nursing Service - KardexDokument4 SeitenIloilo Doctors' College College of Nursing West Avenue, Molo, Iloilo City Nursing Service - KardexKiara Denise TamayoNoch keine Bewertungen
- Group 2 Congestive Heart Failure (Revised)Dokument18 SeitenGroup 2 Congestive Heart Failure (Revised)Florence Dumawal FariñasNoch keine Bewertungen
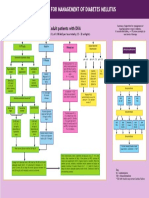
- DM Diabetic Ketoacidosis DKA Management Algorithm Adult Patients 2019Dokument1 SeiteDM Diabetic Ketoacidosis DKA Management Algorithm Adult Patients 2019Hendra AfrilaNoch keine Bewertungen
- PAEDS AVS CASES-With ReferenceDokument9 SeitenPAEDS AVS CASES-With ReferencepainconsulatntkpNoch keine Bewertungen
- Hyperkalaemia Algorithm March 2014Dokument1 SeiteHyperkalaemia Algorithm March 2014ZosmasNoch keine Bewertungen
- Hyperkalaemia Management Guidelines For BWC v1.0 FINALDokument16 SeitenHyperkalaemia Management Guidelines For BWC v1.0 FINALGhina NinditasariNoch keine Bewertungen
- Doctor's Order Phase 2Dokument5 SeitenDoctor's Order Phase 2Renea Joy ArruejoNoch keine Bewertungen
- Protocols ST Helens Adult Sepsis Management PathwayDokument1 SeiteProtocols ST Helens Adult Sepsis Management Pathwayputra purnomoNoch keine Bewertungen
- Rtc-Eeng 2014 10 N Massive Blood LossDokument2 SeitenRtc-Eeng 2014 10 N Massive Blood LossAnisoara AvonNoch keine Bewertungen
- ED Module 4Dokument26 SeitenED Module 4Washi AkunNoch keine Bewertungen
- Hyperkalemia Management Dec2010 PDFDokument6 SeitenHyperkalemia Management Dec2010 PDFClaudia IrimieNoch keine Bewertungen
- Hepatitis A Hepatitis B Hepatitis C Hepatitis D Hepatitis E Hepatitis GDokument9 SeitenHepatitis A Hepatitis B Hepatitis C Hepatitis D Hepatitis E Hepatitis Gjamie carpioNoch keine Bewertungen
- OB Care Plan: Assessment DataDokument9 SeitenOB Care Plan: Assessment Dataapi-520841770Noch keine Bewertungen
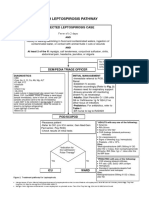
- Leptospirosis Pathway JULY 2018FINALDokument5 SeitenLeptospirosis Pathway JULY 2018FINALNehemiah FranciscoNoch keine Bewertungen
- Doctor-Order-101 Final ChuchuDokument7 SeitenDoctor-Order-101 Final ChuchuJo CardenoNoch keine Bewertungen
- Course of Illness:: ClassificationDokument2 SeitenCourse of Illness:: ClassificationKrista P. AguinaldoNoch keine Bewertungen
- Chief Complain: Jaundice 4/6/5/18:: HB HCT WBC PLT OT PT Alb BUN Creatinin Bil Direk Bil Total PPT ApttDokument8 SeitenChief Complain: Jaundice 4/6/5/18:: HB HCT WBC PLT OT PT Alb BUN Creatinin Bil Direk Bil Total PPT ApttRabiatul 'raney' AdawiyahNoch keine Bewertungen
- Endorsement NotesDokument2 SeitenEndorsement NotesBianca Mikaela DosdosNoch keine Bewertungen
- Doctors Order (Allergy)Dokument4 SeitenDoctors Order (Allergy)Alkiana SalardaNoch keine Bewertungen
- Mariano Marcos State University: College of Health SciencesDokument3 SeitenMariano Marcos State University: College of Health SciencesJoshua GonzalesNoch keine Bewertungen
- Canine Blood Component TableDokument1 SeiteCanine Blood Component TableTrifan PatriciaNoch keine Bewertungen
- Course in The Ward: Date and Time Focus Doctor's Order Nurses Note August 28, 2018 3:50PM Vital Signs: AdmissionDokument4 SeitenCourse in The Ward: Date and Time Focus Doctor's Order Nurses Note August 28, 2018 3:50PM Vital Signs: AdmissionMartin T ManuelNoch keine Bewertungen
- DKA/HHS Pathway Phase 1 (Adult)Dokument6 SeitenDKA/HHS Pathway Phase 1 (Adult)marshaNoch keine Bewertungen
- Nurses' Notes and Treatment Record: Date/Time Focus Progress Notes (D-Data A-Action R-Response)Dokument2 SeitenNurses' Notes and Treatment Record: Date/Time Focus Progress Notes (D-Data A-Action R-Response)Jamie Lee100% (2)
- Cedar Crest College Clinical and Concept Map Worksheet For Nursing 330 PediatricsDokument17 SeitenCedar Crest College Clinical and Concept Map Worksheet For Nursing 330 Pediatricsapi-380115954Noch keine Bewertungen
- Hypoglycaemia FlowchartDokument1 SeiteHypoglycaemia FlowchartMohammad SultanNoch keine Bewertungen
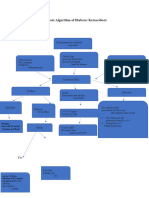
- DKA AlgorismDokument2 SeitenDKA AlgorismYohannes hailuNoch keine Bewertungen
- Adult: Diabetic Emergencies: Care Protocol and ChartDokument4 SeitenAdult: Diabetic Emergencies: Care Protocol and ChartvladhdNoch keine Bewertungen
- TWU Anesthesia Cheat SheetDokument2 SeitenTWU Anesthesia Cheat Sheetinvading_jam7582100% (5)
- DKA Protocol With Calculation SheetDokument7 SeitenDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNoch keine Bewertungen
- POMR ResponsiDokument7 SeitenPOMR ResponsiAcha TuhepalyNoch keine Bewertungen
- Pomr ContohDokument6 SeitenPomr ContohRasyidu MashuriNoch keine Bewertungen
- Endorse PIDokument1 SeiteEndorse PIKUNWAR BRIKSHANoch keine Bewertungen
- Intravenous Insulin Prescription and Fluid Protocol: For Diabetic Keto-Acidosis (Dka)Dokument4 SeitenIntravenous Insulin Prescription and Fluid Protocol: For Diabetic Keto-Acidosis (Dka)sunrise755Noch keine Bewertungen
- Care Plan For GastrectomyDokument16 SeitenCare Plan For GastrectomyPriyal ParikhNoch keine Bewertungen
- Map DkaDokument1 SeiteMap DkaSH PrageethNoch keine Bewertungen
- Critical Care Drug Reference SheetDokument12 SeitenCritical Care Drug Reference SheetYanina CoxNoch keine Bewertungen
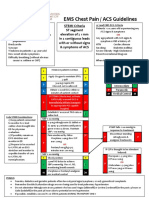
- EMS Chest Pain / ACS GuidelinesDokument1 SeiteEMS Chest Pain / ACS GuidelinesJuanaly BadiolaNoch keine Bewertungen
- NCP-hepatitis-MATA (Risk For Deficient Fluid Volume)Dokument7 SeitenNCP-hepatitis-MATA (Risk For Deficient Fluid Volume)Nicole Keesha MataNoch keine Bewertungen
- New Intern Guide Quick NotesDokument8 SeitenNew Intern Guide Quick NotesTrisNoch keine Bewertungen
- Objective Data Diagnosis Goals Interventions EvaluationDokument2 SeitenObjective Data Diagnosis Goals Interventions EvaluationHira Akram Hira AkramNoch keine Bewertungen
- nsg-320cc Care Plan 1Dokument14 Seitennsg-320cc Care Plan 1api-509452165Noch keine Bewertungen
- NCP ObDokument2 SeitenNCP ObMark Justin LealNoch keine Bewertungen
- NCP FluidDokument4 SeitenNCP FluidSofronio OmboyNoch keine Bewertungen
- Clinical Part A PortfolioDokument11 SeitenClinical Part A Portfolioapi-404111470Noch keine Bewertungen
- Drug Study: Batangas State UniversityDokument8 SeitenDrug Study: Batangas State UniversityFreya Janina ReyesNoch keine Bewertungen
- DKA Adults Management Protocol - DR Anwar Ul HaqDokument3 SeitenDKA Adults Management Protocol - DR Anwar Ul HaqAnwar ul HaqNoch keine Bewertungen
- Diabetes Mellitus TranscribingDokument23 SeitenDiabetes Mellitus TranscribingJasmin B. ERMITANoch keine Bewertungen
- DRUGsssDokument2 SeitenDRUGsssSteffi MurielNoch keine Bewertungen
- ICU Progress NoteDokument7 SeitenICU Progress NoteDiana Hylton100% (1)
- Emergency Treatment of Hyperkalaemia: Protect The HeartDokument1 SeiteEmergency Treatment of Hyperkalaemia: Protect The Heartdilie1992100% (1)
- Aling Marites Case Study:: Endorsement ForDokument4 SeitenAling Marites Case Study:: Endorsement ForTom CuencaNoch keine Bewertungen
- Acute Hepatitis ADokument1 SeiteAcute Hepatitis ACJMALNoch keine Bewertungen
- Peadiatric Advanced Life Support (Pals)Dokument18 SeitenPeadiatric Advanced Life Support (Pals)SREEDEVI T SURESHNoch keine Bewertungen
- Primary Use of Heparin Is To Prevent Venous Thrombosis,: HeparinsDokument2 SeitenPrimary Use of Heparin Is To Prevent Venous Thrombosis,: HeparinsJanna Vivien Prigo BaldioNoch keine Bewertungen
- Angio ChecklistDokument1 SeiteAngio ChecklistZul Hisyam FikriNoch keine Bewertungen
- NCP Sunga Mariane G. BSN4 5Dokument6 SeitenNCP Sunga Mariane G. BSN4 5Erryl Justine AdvinculaNoch keine Bewertungen
- Principles of Management of DKADokument4 SeitenPrinciples of Management of DKAHassen Kavi IsseNoch keine Bewertungen
- Toolbox Talks Working at Elevations English 1Dokument1 SeiteToolbox Talks Working at Elevations English 1AshpakNoch keine Bewertungen
- MÁY 5 Service Manual Bellavista 1000 V16 08Dokument126 SeitenMÁY 5 Service Manual Bellavista 1000 V16 08Huế TrầnNoch keine Bewertungen
- Aoc f22sDokument43 SeitenAoc f22sJoao Jose Santos NetoNoch keine Bewertungen
- Surface & Subsurface Geotechnical InvestigationDokument5 SeitenSurface & Subsurface Geotechnical InvestigationAshok Kumar SahaNoch keine Bewertungen
- Learning Guide: Central Texas College Department of NursingDokument26 SeitenLearning Guide: Central Texas College Department of Nursingapi-3697326Noch keine Bewertungen
- DuctBank For Electrical SystemDokument4 SeitenDuctBank For Electrical SystemAnonymous XYAPaxjbYNoch keine Bewertungen
- 300.91C - Fire Alarm System Pre-Test and Acceptance Test Checklist 3-27-14Dokument2 Seiten300.91C - Fire Alarm System Pre-Test and Acceptance Test Checklist 3-27-14mthuyaNoch keine Bewertungen
- Method Statement - Refrigerant PipingDokument7 SeitenMethod Statement - Refrigerant PipingGirithar M SundaramNoch keine Bewertungen
- Flooding Deagon Flood Flag MapDokument1 SeiteFlooding Deagon Flood Flag MapNgaire TaylorNoch keine Bewertungen
- Intro To BiochemDokument2 SeitenIntro To BiochemPeachy PieNoch keine Bewertungen
- 8 Field Quality PlanDokument18 Seiten8 Field Quality PlanRamaKrishna ANoch keine Bewertungen
- Conversion Tables by Cafe Fernando Food BlogDokument5 SeitenConversion Tables by Cafe Fernando Food BlogElston FooNoch keine Bewertungen
- Ficha-Tecnica-Tuberia MechDokument2 SeitenFicha-Tecnica-Tuberia MechCarlos salazarNoch keine Bewertungen
- 510 1453 1 PB Tiang ReklameDokument6 Seiten510 1453 1 PB Tiang ReklameGunaedy UtomoNoch keine Bewertungen
- Chapter 1 Cumulative Review: Multiple ChoiceDokument2 SeitenChapter 1 Cumulative Review: Multiple ChoiceJ. LeeNoch keine Bewertungen
- University of LeedsDokument20 SeitenUniversity of LeedsYasir KhanNoch keine Bewertungen
- List of Irc Publications Referred To in The Specifications: AppendicesDokument17 SeitenList of Irc Publications Referred To in The Specifications: AppendicesPrasad BoniNoch keine Bewertungen
- Lesson 2 Arts of East AsiaDokument21 SeitenLesson 2 Arts of East Asiarenaldo ocampoNoch keine Bewertungen
- Oc818 Manual v03-1Dokument5 SeitenOc818 Manual v03-1Luca PayetNoch keine Bewertungen
- Orchestral Recording, January 2006Dokument10 SeitenOrchestral Recording, January 2006Rhys WilliamsNoch keine Bewertungen
- Reason: God Had Made The Mistake of Sending Only 70 PesosDokument2 SeitenReason: God Had Made The Mistake of Sending Only 70 PesosS Vaibhav81% (21)
- SpeedFace M4 DatasheetDokument2 SeitenSpeedFace M4 DatasheetRENJITH K NAIRNoch keine Bewertungen
- Rockwell Allen BradleyDokument73 SeitenRockwell Allen BradleymaygomezNoch keine Bewertungen
- AT2H - Basics - Symbolism in HinduismDokument28 SeitenAT2H - Basics - Symbolism in Hinduismapi-3764210Noch keine Bewertungen
- Barilla SpaDokument11 SeitenBarilla Spavariapratik100% (1)
- Integration of Phodi Process With Mutation in Bhoomi (Simultaneous Approval of Phodi and The Mutation)Dokument19 SeitenIntegration of Phodi Process With Mutation in Bhoomi (Simultaneous Approval of Phodi and The Mutation)seshadrimn seshadrimnNoch keine Bewertungen
- Local AnesthesiaDokument55 SeitenLocal AnesthesiaAhmed MagdyNoch keine Bewertungen
- Genesis of KupferschieferDokument15 SeitenGenesis of KupferschieferMaricela GarciaNoch keine Bewertungen
- LH514 - OkokDokument6 SeitenLH514 - OkokVictor Yañez Sepulveda100% (1)
- MFI 2 - Unit 3 - SB - L+SDokument10 SeitenMFI 2 - Unit 3 - SB - L+SHoan HoàngNoch keine Bewertungen