Das könnte Ihnen auch gefallen
- Stepping On CertificateDokument1 SeiteStepping On Certificateapi-262531856Noch keine Bewertungen
- Addressing Cognition and Executive Function in Patients With Tbi & AbiDokument40 SeitenAddressing Cognition and Executive Function in Patients With Tbi & Abiapi-262531856Noch keine Bewertungen
- Resume With No Contact Info PubDokument2 SeitenResume With No Contact Info Pubapi-262531856Noch keine Bewertungen
- Goddard Occupational Analysis & Intervention PlanDokument23 SeitenGoddard Occupational Analysis & Intervention Planapi-262531856Noch keine Bewertungen
- Treating Baby B - A Jeune Syndrome Case StudyDokument21 SeitenTreating Baby B - A Jeune Syndrome Case Studyapi-262531856Noch keine Bewertungen
- Reflection On LeadershipDokument2 SeitenReflection On Leadershipapi-262531856Noch keine Bewertungen
- Reflection On Occupation-Based PracticeDokument2 SeitenReflection On Occupation-Based Practiceapi-262531856Noch keine Bewertungen
- Coordinated Intake Info Sheet Help Hope HomeDokument2 SeitenCoordinated Intake Info Sheet Help Hope Homeapi-262531856Noch keine Bewertungen
- HSH EvalDokument5 SeitenHSH Evalapi-262531856Noch keine Bewertungen
- Reflection On Evidence-Based PracticeDokument2 SeitenReflection On Evidence-Based Practiceapi-262531856Noch keine Bewertungen
- Reflection On Social JusticeDokument2 SeitenReflection On Social Justiceapi-262531856Noch keine Bewertungen
- Ncep EvalDokument4 SeitenNcep Evalapi-262531856Noch keine Bewertungen
- Leadership Development PlanDokument5 SeitenLeadership Development Planapi-262531856Noch keine Bewertungen
- Nevada Resources For Homeless ResidentsDokument2 SeitenNevada Resources For Homeless Residentsapi-262531856Noch keine Bewertungen
- Research Day-Nidcap - Goddard & Noss 2015Dokument16 SeitenResearch Day-Nidcap - Goddard & Noss 2015api-262531856Noch keine Bewertungen
- Nota PresenterDokument1 SeiteNota Presenterapi-262531856Noch keine Bewertungen
- Sunrise Level II EvalDokument8 SeitenSunrise Level II Evalapi-262531856Noch keine Bewertungen
- Opportunity Village EvalDokument5 SeitenOpportunity Village Evalapi-262531856Noch keine Bewertungen
- Cat Worksheet - Nidcap - Goddard & Noss FinalDokument11 SeitenCat Worksheet - Nidcap - Goddard & Noss Finalapi-262531856Noch keine Bewertungen
- Ccls CertificateDokument1 SeiteCcls Certificateapi-262531856Noch keine Bewertungen
- Pte PresidentDokument1 SeitePte Presidentapi-262531856Noch keine Bewertungen
- Home Assessment DocumentDokument8 SeitenHome Assessment Documentapi-262531856Noch keine Bewertungen
- Addressing Cognition Poster 36x42Dokument1 SeiteAddressing Cognition Poster 36x42api-262531856Noch keine Bewertungen
- Pi Theta InitiationDokument1 SeitePi Theta Initiationapi-262531856Noch keine Bewertungen
- Activities For Book PDF VersionDokument12 SeitenActivities For Book PDF Versionapi-262531856Noch keine Bewertungen
- Nidcap Poster Final Edited For Research DayDokument1 SeiteNidcap Poster Final Edited For Research Dayapi-262531856Noch keine Bewertungen
- Cat Evidence Table - Nidcap - Goddard & Noss Final 1 in MarginsDokument28 SeitenCat Evidence Table - Nidcap - Goddard & Noss Final 1 in Marginsapi-262531856Noch keine Bewertungen
- Evidence Paper On Adolescent Transitional ProgramsDokument14 SeitenEvidence Paper On Adolescent Transitional Programsapi-262531856Noch keine Bewertungen
- Not Anymore Certificate of CompletionDokument1 SeiteNot Anymore Certificate of Completionapi-262531856Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Is It Simple To Explain Simple Experiments The Heavy Newspaper' Stick BreakDokument6 SeitenIs It Simple To Explain Simple Experiments The Heavy Newspaper' Stick Break이온유Noch keine Bewertungen
- MPLS QAsDokument6 SeitenMPLS QAsLaxman Shrestha100% (1)
- CE 205 - Analyzing Hydrographs and Deriving Unit HydrographsDokument17 SeitenCE 205 - Analyzing Hydrographs and Deriving Unit HydrographsUmange RanasingheNoch keine Bewertungen
- Powercrete R95Dokument2 SeitenPowercrete R95Jimmy CalderonNoch keine Bewertungen
- CmeDokument41 SeitenCmekhalis@hotmail.com100% (1)
- VDVDVXVCFDBCVCDokument390 SeitenVDVDVXVCFDBCVCHafiz Rahmat UllahNoch keine Bewertungen
- Bio PharmaceuticsDokument48 SeitenBio PharmaceuticsRajan Kashyap100% (2)
- DefinitionsHypothesesPosterior Analytics (Landor)Dokument12 SeitenDefinitionsHypothesesPosterior Analytics (Landor)Daniel Rojas UNoch keine Bewertungen
- B483B483M 13e1Dokument10 SeitenB483B483M 13e1Mohamad ZandiNoch keine Bewertungen
- UI5 TrainingDokument110 SeitenUI5 TrainingShailesh KumarNoch keine Bewertungen
- Sal de CrosetatDokument3 SeitenSal de CrosetatMădălina Pisău100% (1)
- ES Q2 Mod8Dokument26 SeitenES Q2 Mod8maacovsNoch keine Bewertungen
- Hassāniyya Arabic DialectDokument15 SeitenHassāniyya Arabic DialectTiddukla Tadelsant Imedyazen100% (1)
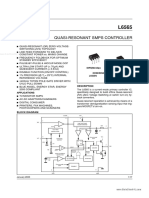
- L6565 DatasheetDokument17 SeitenL6565 DatasheetJose BenavidesNoch keine Bewertungen
- 0620 Chemistry: MARK SCHEME For The March 2015 SeriesDokument6 Seiten0620 Chemistry: MARK SCHEME For The March 2015 SeriesDark GreenNoch keine Bewertungen
- 5.1.2. Biological Indicators of SterilisationDokument1 Seite5.1.2. Biological Indicators of SterilisationSurendar KesavanNoch keine Bewertungen
- Control Charts For Lognormal DataDokument7 SeitenControl Charts For Lognormal Dataanjo0225Noch keine Bewertungen
- Sterlization of Water Using Bleaching Powder PDFDokument20 SeitenSterlization of Water Using Bleaching Powder PDFradha krishnanNoch keine Bewertungen
- Micro Shelter Product Description V5aDokument11 SeitenMicro Shelter Product Description V5aIan JaredNoch keine Bewertungen
- GH Chap 78 - Insulin, Glucagon and DMDokument16 SeitenGH Chap 78 - Insulin, Glucagon and DMShellz2428Noch keine Bewertungen
- Oracle Database - Introduction To SQL Ed 2Dokument5 SeitenOracle Database - Introduction To SQL Ed 2Miguel Alfonso DIAZ MORRISNoch keine Bewertungen
- CH-2 Earth DamsDokument18 SeitenCH-2 Earth DamssidNoch keine Bewertungen
- Vendor Information Vishay BLH Handbook TC0013 Solutions For Process Weighing and Force Measurement Electronic Weigh SystemsDokument59 SeitenVendor Information Vishay BLH Handbook TC0013 Solutions For Process Weighing and Force Measurement Electronic Weigh SystemsAndrew JacksonNoch keine Bewertungen
- Check List For Overall Piping Plot PlanDokument3 SeitenCheck List For Overall Piping Plot PlankamleshyadavmoneyNoch keine Bewertungen
- MCQ Metrology (CCCM & CCCT) PDFDokument21 SeitenMCQ Metrology (CCCM & CCCT) PDFSahil Gauhar67% (3)
- Session5 Automotive PackagingDokument72 SeitenSession5 Automotive PackagingShivprasad Savadatti100% (1)
- SUDOKU DocumentDokument37 SeitenSUDOKU DocumentAmbika Sharma33% (3)
- UntitledDokument135 SeitenUntitledtaraji dawlaNoch keine Bewertungen
- St. Michael'S High SchoolDokument5 SeitenSt. Michael'S High SchoolHoniel PagoboNoch keine Bewertungen
- BasrahDokument19 SeitenBasrahDurban Chamber of Commerce and IndustryNoch keine Bewertungen