Das könnte Ihnen auch gefallen
- Science Magazine February 2020Dokument133 SeitenScience Magazine February 2020Elena González GonzálezNoch keine Bewertungen
- List of Fatigue Standards and Fracture Standards Developed by ASTM & ISODokument3 SeitenList of Fatigue Standards and Fracture Standards Developed by ASTM & ISOSatrio Aditomo100% (1)
- HERNIORRHAPHYDokument2 SeitenHERNIORRHAPHYSheldon Deypalubos Jr.Noch keine Bewertungen
- 01-20 Optical Multiplexer and Demultiplexer BoardDokument57 Seiten01-20 Optical Multiplexer and Demultiplexer BoardDaler ShorahmonovNoch keine Bewertungen
- Mastectomy (Case Analysis)Dokument7 SeitenMastectomy (Case Analysis)Lester_Ocuaman_2248Noch keine Bewertungen
- LaparotomyDokument36 SeitenLaparotomydenekeNoch keine Bewertungen
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- NCP-fluid Volume DeficitDokument4 SeitenNCP-fluid Volume DeficitChrissa Mae Aranilla MayoNoch keine Bewertungen
- Dave Jay S. Manriquez RN. Acute CholecystitisDokument11 SeitenDave Jay S. Manriquez RN. Acute CholecystitisChilleMaeNoch keine Bewertungen
- Iec60227-3 (Ed2.1) en DDokument6 SeitenIec60227-3 (Ed2.1) en Duntuk donlod aaaNoch keine Bewertungen
- Esophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNDokument20 SeitenEsophagea L Cancer: By: Krizzia S. Bunagan-Legasi, RNAnn SalvatierraNoch keine Bewertungen
- Modified Radical MastectomyDokument6 SeitenModified Radical Mastectomymetch isulatNoch keine Bewertungen
- Scribd 020922 Case Study-Oncology A&kDokument2 SeitenScribd 020922 Case Study-Oncology A&kKellie DNoch keine Bewertungen
- Urinalysis: PurposeDokument6 SeitenUrinalysis: PurposebobtagubaNoch keine Bewertungen
- NCP FeuDokument2 SeitenNCP FeuFejlean Angelica AntineoNoch keine Bewertungen
- Pathophysiology of Acute PancreatitisDokument1 SeitePathophysiology of Acute PancreatitisHarvin FrancoNoch keine Bewertungen
- COVID-19: Brian, Fernando, Jason, FelitaDokument8 SeitenCOVID-19: Brian, Fernando, Jason, FelitaCharson ChenNoch keine Bewertungen
- TahbsoDokument4 SeitenTahbsomichZ_13Noch keine Bewertungen
- Solutions: 1 US A Te CareDokument2 SeitenSolutions: 1 US A Te CareelonaNoch keine Bewertungen
- Case Study MastectomyDokument26 SeitenCase Study MastectomyIcheAnne Nilay100% (2)
- Hyperosmolar Hyperglycemic State (HHS)Dokument21 SeitenHyperosmolar Hyperglycemic State (HHS)Malueth AnguiNoch keine Bewertungen
- Acute Pancreatitis - Practice Essentials, Background, PathophysiologyDokument18 SeitenAcute Pancreatitis - Practice Essentials, Background, PathophysiologyInês BipNoch keine Bewertungen
- TriageDokument8 SeitenTriageSarah GuintoNoch keine Bewertungen
- Metabolism Case StudiesDokument3 SeitenMetabolism Case StudiesEpoy Bantawig0% (1)
- Bladder CancerDokument1 SeiteBladder CancerCarmina AguilarNoch keine Bewertungen
- Myasthenia GravisDokument16 SeitenMyasthenia Graviszarka wahid buxNoch keine Bewertungen
- Occurs Most Often In:: Muscular DystrophyDokument4 SeitenOccurs Most Often In:: Muscular DystrophyJiezl Abellano AfinidadNoch keine Bewertungen
- OsteomyelitisDokument7 SeitenOsteomyelitis4kscribd100% (1)
- Nursing Care Plan: Subjective CuesDokument2 SeitenNursing Care Plan: Subjective CuesNicole cuencosNoch keine Bewertungen
- Buerger's DiseaseDokument5 SeitenBuerger's Diseaseglie_e52164100% (5)
- B00K 3 Unit 13Dokument11 SeitenB00K 3 Unit 13Rolli SptNoch keine Bewertungen
- NCP Ko BabyDokument3 SeitenNCP Ko BabyDaniel ApostolNoch keine Bewertungen
- Case Study ReportDokument23 SeitenCase Study Reportapi-290866384Noch keine Bewertungen
- Discharge Planning EnglishDokument11 SeitenDischarge Planning Englishrahmat hidayatNoch keine Bewertungen
- Acute Pain - Mastectomy - Breast CADokument2 SeitenAcute Pain - Mastectomy - Breast CAAngie MandeoyaNoch keine Bewertungen
- HemorrhoidectomyDokument5 SeitenHemorrhoidectomydrnareshkumar3281100% (1)
- Nursing Care Plan For Angina Pectoris NCPDokument2 SeitenNursing Care Plan For Angina Pectoris NCPkarthi karthi100% (1)
- Pulmonary EmbolismDokument46 SeitenPulmonary EmbolismAnusha VergheseNoch keine Bewertungen
- Pathophysiology of Transitional Cell CarcinomaDokument10 SeitenPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansNoch keine Bewertungen
- Case Study StabDokument7 SeitenCase Study StabMari Jasmeen Estrada Noveda100% (1)
- Diarrhea Care PlanDokument2 SeitenDiarrhea Care Planzepoli_zepoly6232100% (1)
- HNPDokument7 SeitenHNPLyka Mae Imbat - Pacnis100% (1)
- ThyroidectomyDokument51 SeitenThyroidectomyPopey Moore100% (1)
- Classification of Instruments and It's RecDokument48 SeitenClassification of Instruments and It's RecLeni CarununganNoch keine Bewertungen
- End Stage Renal DiseaseDokument9 SeitenEnd Stage Renal DiseaseShantanu DixitNoch keine Bewertungen
- Ineffective Tissue PerfusionDokument5 SeitenIneffective Tissue PerfusionKryza Dale Bunado BaticanNoch keine Bewertungen
- TAHBSO ReportDokument4 SeitenTAHBSO ReportsachiiMeNoch keine Bewertungen
- Impaired Physical Mobility R/T Neuromuscular ImpairmentDokument3 SeitenImpaired Physical Mobility R/T Neuromuscular ImpairmentjisooNoch keine Bewertungen
- Percutaneous Endoscopic GastrostomyDokument27 SeitenPercutaneous Endoscopic GastrostomyDoha EbedNoch keine Bewertungen
- ThyroidectomyDokument2 SeitenThyroidectomykzone2290Noch keine Bewertungen
- Pathophysiology of AppendicitisDokument2 SeitenPathophysiology of AppendicitisSherry Mae Rizza GonzalesNoch keine Bewertungen
- Appendectomy Case PresentationDokument23 SeitenAppendectomy Case PresentationMarie Nelle Escriba LimpocoNoch keine Bewertungen
- NCP For Impaired Oral Mucous MembraneDokument11 SeitenNCP For Impaired Oral Mucous MembraneRYAN SAPLADNoch keine Bewertungen
- Drug StudyDokument8 SeitenDrug StudyJohn Ronald P. RamosNoch keine Bewertungen
- NCP CKDDokument3 SeitenNCP CKDRiel TumandaNoch keine Bewertungen
- Student Nurses' Community: NURSING CARE PLAN Functional Urinary IncontinenceDokument4 SeitenStudent Nurses' Community: NURSING CARE PLAN Functional Urinary IncontinenceJez RarangNoch keine Bewertungen
- CholelithiasisDokument3 SeitenCholelithiasisMIlanSagittarius0% (1)
- Case Study Ugib Lower MBDokument65 SeitenCase Study Ugib Lower MBQuolette Constante100% (1)
- NCPDokument3 SeitenNCPLuiji Amor TiamzonNoch keine Bewertungen
- Ch42 NCP IneffectiveCoping 1075-1076Dokument2 SeitenCh42 NCP IneffectiveCoping 1075-1076Dizerine Mirafuentes RolidaNoch keine Bewertungen
- Assessment Diagnosis Planning Intervention Rationale EvaluationDokument1 SeiteAssessment Diagnosis Planning Intervention Rationale EvaluationFranz RolfNoch keine Bewertungen
- NCPDokument3 SeitenNCPErica Denice CastilloNoch keine Bewertungen
- Exploratory LaparotomyDokument25 SeitenExploratory Laparotomywinai13Noch keine Bewertungen
- CHOLECYSTECTOMYDokument6 SeitenCHOLECYSTECTOMYRaymond Sabanal BanquirigoNoch keine Bewertungen
- Javanese PeopleDokument22 SeitenJavanese PeopleDenisaNoch keine Bewertungen
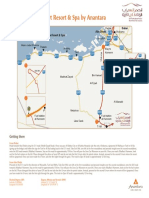
- Qasr Al Sarab Desert Resort Location Map June2012Dokument1 SeiteQasr Al Sarab Desert Resort Location Map June2012Anant GârgNoch keine Bewertungen
- Frye LGD As A Function of The Default Rate 091013 PDFDokument13 SeitenFrye LGD As A Function of The Default Rate 091013 PDFSushant SinghNoch keine Bewertungen
- Practice For Mounting Buses & Joints-374561Dokument11 SeitenPractice For Mounting Buses & Joints-374561a_sengar1Noch keine Bewertungen
- Chillers VoltasDokument4 SeitenChillers Voltasanil shuklaNoch keine Bewertungen
- English Class Vii PDFDokument101 SeitenEnglish Class Vii PDFpannapurohitNoch keine Bewertungen
- Lima Indiana Oil FieldDokument32 SeitenLima Indiana Oil FieldCHARLES PATULAYNoch keine Bewertungen
- Petersen Coils Basic 20principle and ApplicationDokument3 SeitenPetersen Coils Basic 20principle and ApplicationasotozuazuaNoch keine Bewertungen
- Free Electron TheoryDokument8 SeitenFree Electron TheoryNeelam KapoorNoch keine Bewertungen
- Precision CatalogDokument256 SeitenPrecision CatalogImad AghilaNoch keine Bewertungen
- Phrasal Verbs Related To HealthDokument2 SeitenPhrasal Verbs Related To HealthKnuckles El Naco Narco LechugueroNoch keine Bewertungen
- Statics: Vector Mechanics For EngineersDokument39 SeitenStatics: Vector Mechanics For EngineersVijay KumarNoch keine Bewertungen
- English2 Q2 Summative Assessment 4 2Dokument4 SeitenEnglish2 Q2 Summative Assessment 4 2ALNIE PANGANIBANNoch keine Bewertungen
- GBJ0232 - en GLX 3101 T2Dokument43 SeitenGBJ0232 - en GLX 3101 T2mnbvqwert100% (2)
- AIR Conditioner: Owner'S ManualDokument52 SeitenAIR Conditioner: Owner'S Manualashley diazNoch keine Bewertungen
- Manuscript FsDokument76 SeitenManuscript FsRalph HumpaNoch keine Bewertungen
- ff2023 Web 0 0Dokument2 Seitenff2023 Web 0 0khaing khantNoch keine Bewertungen
- Wildlife Emergency and Critical CareDokument14 SeitenWildlife Emergency and Critical CareRayssa PereiraNoch keine Bewertungen
- RepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUDokument2 SeitenRepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUPR.comNoch keine Bewertungen
- Welcome To Our 2Nd Topic: History of VolleyballDokument6 SeitenWelcome To Our 2Nd Topic: History of VolleyballDharyn KhaiNoch keine Bewertungen
- Wcdma Idle Mode (Ericsson)Dokument29 SeitenWcdma Idle Mode (Ericsson)Hosein ShahbaziNoch keine Bewertungen
- Basics of Population EducationDokument4 SeitenBasics of Population EducationLAILANIE DELA PENANoch keine Bewertungen
- Bchem 455 - Module 3Dokument42 SeitenBchem 455 - Module 3WilliamNoch keine Bewertungen
- 3M Novec 1230 Fire Protection Fluid FAQDokument8 Seiten3M Novec 1230 Fire Protection Fluid FAQEden CansonNoch keine Bewertungen
- End of Summer Course Test August 2021Dokument16 SeitenEnd of Summer Course Test August 2021Thanh Nguyen vanNoch keine Bewertungen
- 2017 Classification of Periodontal and Peri-Implant Diseases and Conditions. Decision Making Algorithms For Clinical PracticeDokument40 Seiten2017 Classification of Periodontal and Peri-Implant Diseases and Conditions. Decision Making Algorithms For Clinical PracticebbNoch keine Bewertungen