Das könnte Ihnen auch gefallen
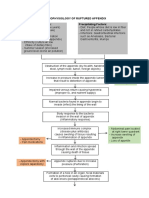
- Pathophysiology of Ruptured AppendixDokument2 SeitenPathophysiology of Ruptured AppendixAya PaquitNoch keine Bewertungen
- Appendix 1 Occupational Therapy Bathing-Showering ToolDokument3 SeitenAppendix 1 Occupational Therapy Bathing-Showering ToolNizam lotfiNoch keine Bewertungen
- Multiple Physical Injuries Secondary To Vehicular AccidentDokument31 SeitenMultiple Physical Injuries Secondary To Vehicular AccidentAnton Laurenciana50% (2)
- Case - Neck MassDokument78 SeitenCase - Neck MassMico TanNoch keine Bewertungen
- Post Anaesthesia Shivering - N PadayacheeDokument19 SeitenPost Anaesthesia Shivering - N Padayacheexxxvrgnt100% (2)
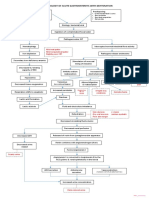
- Pathophysiology of Gastric Cancer Precipitating Factors: - Predisposing FactorsDokument3 SeitenPathophysiology of Gastric Cancer Precipitating Factors: - Predisposing FactorsJu Lie AnnNoch keine Bewertungen
- 2018 Doh Ambulance License RequirementsDokument31 Seiten2018 Doh Ambulance License RequirementsChris-Goldie Lorezo87% (31)
- NCP LeptospirosisDokument2 SeitenNCP LeptospirosisLouise Anne Asuncion OclimaNoch keine Bewertungen
- Pulmonary Tuberculosis: A Case Study ofDokument33 SeitenPulmonary Tuberculosis: A Case Study ofRJ MarquezNoch keine Bewertungen
- Chron's Disease 2Dokument3 SeitenChron's Disease 2TarantadoNoch keine Bewertungen
- Handout IV: DSM-5 ASD Checklist: Making An Autism Spectrum Disorder DiagnosisDokument2 SeitenHandout IV: DSM-5 ASD Checklist: Making An Autism Spectrum Disorder DiagnosisValentina IerotheouNoch keine Bewertungen
- Operating Room Write-Up: PathophysiologyDokument4 SeitenOperating Room Write-Up: PathophysiologyArian May MarcosNoch keine Bewertungen
- Pathophysiology of AGE With DHNDokument1 SeitePathophysiology of AGE With DHNFarr Krizha Tangkusan50% (2)
- 3 Developmental Tasks of Later MaturityDokument3 Seiten3 Developmental Tasks of Later MaturitySarah BenjaminNoch keine Bewertungen
- Jurisprudence RevDokument48 SeitenJurisprudence RevJoel JoseNoch keine Bewertungen
- NeuroMuscular Blocking AgentsDokument3 SeitenNeuroMuscular Blocking AgentsdrugdrugNoch keine Bewertungen
- Ondansetron (Zofran)Dokument1 SeiteOndansetron (Zofran)Cassie100% (1)
- Autonomic Nervous System PharmacologyDokument7 SeitenAutonomic Nervous System Pharmacologydonordarah93Noch keine Bewertungen
- Cellular AberrationDokument14 SeitenCellular AberrationjinahyangNoch keine Bewertungen
- Dental Case Sheet Corrcted / Orthodontic Courses by Indian Dental AcademyDokument8 SeitenDental Case Sheet Corrcted / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- Pathophysiology of Rheumatic FeverDokument3 SeitenPathophysiology of Rheumatic FeverGehlatin Tumanan100% (2)
- NAPREXDokument2 SeitenNAPREXKarl EdemNoch keine Bewertungen
- B. Diagram: Predisposing Factors: Precipitating Factors EtiologyDokument3 SeitenB. Diagram: Predisposing Factors: Precipitating Factors EtiologyKenneth Torres100% (1)
- Pediatric Community Acquired Pneumonia (PCAP) : Case StudyDokument38 SeitenPediatric Community Acquired Pneumonia (PCAP) : Case StudyAndrew Perez0% (1)
- Naprex Drug StudyDokument3 SeitenNaprex Drug StudyAngelica shane NavarroNoch keine Bewertungen
- Afinidad, Jiezl A: Davao Doctors College Nursing ProgramDokument4 SeitenAfinidad, Jiezl A: Davao Doctors College Nursing ProgramJiezl Abellano AfinidadNoch keine Bewertungen
- OR Write Up - Repeat LSCSDokument2 SeitenOR Write Up - Repeat LSCSWyen CabatbatNoch keine Bewertungen
- Patient 3 NSDDokument20 SeitenPatient 3 NSDBea Bianca CruzNoch keine Bewertungen
- Case PresDokument5 SeitenCase PresBeverlyNoch keine Bewertungen
- Drug StudyDokument12 SeitenDrug StudyAnne Marie Angelica BilonoNoch keine Bewertungen
- Final Case Study PCAPDokument72 SeitenFinal Case Study PCAPKelly Tayag100% (1)
- 4.0 Doctors Order Grand CaseDokument23 Seiten4.0 Doctors Order Grand CasekeithNoch keine Bewertungen
- Acute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsDokument3 SeitenAcute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsKyla ValenciaNoch keine Bewertungen
- Pcap PathophysiologyDokument3 SeitenPcap PathophysiologyZandra Lyn AlundayNoch keine Bewertungen
- Nursing Care Plan For Dengue Hemmorrhagic FeverDokument6 SeitenNursing Care Plan For Dengue Hemmorrhagic FeverMean Elepaño100% (1)
- KASP Package RateDokument502 SeitenKASP Package RateAnoop VijayakumarNoch keine Bewertungen
- DengueDokument4 SeitenDengueKathleen DimacaliNoch keine Bewertungen
- NCP of MGH PatientDokument2 SeitenNCP of MGH PatientMaverick LimNoch keine Bewertungen
- Narrative PathophysiologyDokument1 SeiteNarrative PathophysiologyJemsMei Comparativo MensuradoNoch keine Bewertungen
- PATHOPHYSIOLOGY TCHI Client BasedDokument1 SeitePATHOPHYSIOLOGY TCHI Client BasedGem MarasiganNoch keine Bewertungen
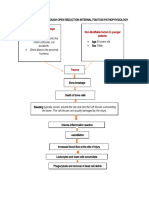
- Post Open Reduction Internal Fixation PathophysiologyDokument3 SeitenPost Open Reduction Internal Fixation PathophysiologyRizalyn QuindipanNoch keine Bewertungen
- Nursing Health HistoryDokument2 SeitenNursing Health HistorySheryhan Tahir BayleNoch keine Bewertungen
- Pcap Pathophysiology PDFDokument3 SeitenPcap Pathophysiology PDFMikaela RamosNoch keine Bewertungen
- PDF Albumin Drug StudyDokument1 SeitePDF Albumin Drug StudyJamie John EsplanadaNoch keine Bewertungen
- Ineffective Health MaintenanceDokument6 SeitenIneffective Health MaintenanceRYAN SAPLADNoch keine Bewertungen
- You Are Caring For A Patient With An NG Feeding TubeDokument2 SeitenYou Are Caring For A Patient With An NG Feeding TubeWen Silver100% (1)
- NCP & Drugstudy FormatDokument7 SeitenNCP & Drugstudy Formatanonymous89ify100% (1)
- Charting CraniotomyDokument1 SeiteCharting CraniotomyJrBong SemaneroNoch keine Bewertungen
- University of Northern PhilippinesDokument2 SeitenUniversity of Northern PhilippinesCezanne Cruz0% (1)
- Cristobal, Rocelyn P. MS Lec Post Task Triage FinalDokument10 SeitenCristobal, Rocelyn P. MS Lec Post Task Triage FinalRocelyn CristobalNoch keine Bewertungen
- Measles PathophysiologyDokument1 SeiteMeasles PathophysiologyAl TheóNoch keine Bewertungen
- DRUG+STUDY NaprexDokument2 SeitenDRUG+STUDY NaprexJoevence Gazo CuaresmaNoch keine Bewertungen
- Assessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationDokument6 SeitenAssessment/ Cues Nursing Diagnosis Background Knowledge Goal and Objectives Nursing Interventions and Rationale EvaluationimnasNoch keine Bewertungen
- Patho Pott's DseDokument2 SeitenPatho Pott's Dsexai_teovisioNoch keine Bewertungen
- OB Group 1 PA ToolDokument23 SeitenOB Group 1 PA ToolAubrey Dynise C. TorralbaNoch keine Bewertungen
- Balance Skeletal TractionDokument5 SeitenBalance Skeletal TractionRachel Ann JimenezNoch keine Bewertungen
- Pathophysiology - AppendicitisDokument5 SeitenPathophysiology - AppendicitisAzielle Joyce RosquetaNoch keine Bewertungen
- DOCTORS ORDER CRMCDokument2 SeitenDOCTORS ORDER CRMCMarielle ChuaNoch keine Bewertungen
- Pathophysiology AGEDokument2 SeitenPathophysiology AGEMareeze Hatta100% (1)
- Gordon's HisDokument4 SeitenGordon's HisJee ShangNoch keine Bewertungen
- Azithromycin Drug StudyDokument2 SeitenAzithromycin Drug StudySHEILA MAE SACLOTNoch keine Bewertungen
- 13-Areas-of-Assessment-2017 2Dokument3 Seiten13-Areas-of-Assessment-2017 2Alyssa Moutrie Dulay ArabeNoch keine Bewertungen
- Case Study - LeptospirosisDokument3 SeitenCase Study - LeptospirosisMarie Jennifer ParilNoch keine Bewertungen
- Geographical Area - Tropical Islands in Thepacific (Philippines) and AsiaDokument1 SeiteGeographical Area - Tropical Islands in Thepacific (Philippines) and AsiaGenevang SeaweedsNoch keine Bewertungen
- PCAP CPDokument14 SeitenPCAP CPMikael R. SmileNoch keine Bewertungen
- Pathophysiology VolvulusDokument2 SeitenPathophysiology VolvulusHyacinth Bueser Bondad0% (2)
- Interview Guide For Nursing Health HistoryDokument3 SeitenInterview Guide For Nursing Health HistoryDersly LaneNoch keine Bewertungen
- CasepresDokument3 SeitenCasepresJoyce Ramos CadondonNoch keine Bewertungen
- Irene's Care StudyDokument68 SeitenIrene's Care StudyLawrence AckahNoch keine Bewertungen
- April LeDokument21 SeitenApril LeAprille Anne SagmitNoch keine Bewertungen
- Chapter 6 Confidence Interval Estimates SolutionDokument18 SeitenChapter 6 Confidence Interval Estimates SolutionShrey Mangal92% (12)
- Aritmia AHA 2017Dokument120 SeitenAritmia AHA 2017Corticosteroids MobileLegendNoch keine Bewertungen
- Drug Study (Cervical Polyp)Dokument4 SeitenDrug Study (Cervical Polyp)aerondominicbasilioNoch keine Bewertungen
- Chrisanthopoulos Marika 300453 Cleft Lip and PalateDokument14 SeitenChrisanthopoulos Marika 300453 Cleft Lip and PalateCharles IppolitoNoch keine Bewertungen
- Formulary - Good ReadDokument121 SeitenFormulary - Good ReadJananiRajamanickamNoch keine Bewertungen
- RhinosporidiosisDokument9 SeitenRhinosporidiosisDrAnwar MKNoch keine Bewertungen
- Standardizing Standard Operating Procedures SOP MDokument3 SeitenStandardizing Standard Operating Procedures SOP MTejasNoch keine Bewertungen
- PSYCHIATRY Classification of Psychiatric Disorder (Dr. Rosal)Dokument11 SeitenPSYCHIATRY Classification of Psychiatric Disorder (Dr. Rosal)Valcrist BalderNoch keine Bewertungen
- 2007 Tweed ProfileDokument60 Seiten2007 Tweed ProfileYeny Valdivia AlbornozNoch keine Bewertungen
- Short WaveDokument31 SeitenShort WaveDharmesh MaheshwariNoch keine Bewertungen
- WelchAllyn Propaq Encore Vital Signs Monitor - Reference GuideDokument178 SeitenWelchAllyn Propaq Encore Vital Signs Monitor - Reference GuideSergio PérezNoch keine Bewertungen
- Carefusion CannulasDokument8 SeitenCarefusion Cannulasrubenr25Noch keine Bewertungen
- DR Ahmed Abar CVDokument7 SeitenDR Ahmed Abar CVAnonymous H1EZvy1yQNoch keine Bewertungen
- Adrenergic Antagonists EditedDokument60 SeitenAdrenergic Antagonists EditedJohn Benedict VocalesNoch keine Bewertungen
- Canine Elbow Dysplasia: Heidi Reuss-Lamky, LVT, VTS (Anesthesia)Dokument6 SeitenCanine Elbow Dysplasia: Heidi Reuss-Lamky, LVT, VTS (Anesthesia)Katarina SimicicNoch keine Bewertungen
- Therapeutic Drug MonitoringDokument6 SeitenTherapeutic Drug MonitoringEdi Uchiha SutarmantoNoch keine Bewertungen
- Leading Dentist in Oshawa - Scarborough - Grandview Dental ClinicDokument7 SeitenLeading Dentist in Oshawa - Scarborough - Grandview Dental Clinicnaveen bansalNoch keine Bewertungen
- Pharmaceutical Sales & Marketing Legal and Ethical ConsiderationsDokument41 SeitenPharmaceutical Sales & Marketing Legal and Ethical ConsiderationsqmnwebNoch keine Bewertungen
- Nursing EducationDokument136 SeitenNursing EducationNishi Vaibhav KumarNoch keine Bewertungen
- By Dr. Myra C. BritillerDokument72 SeitenBy Dr. Myra C. BritillerCharleneBunquin100% (1)