Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Standard Method For Making and Curing Cubes Made From Pre-Bagged Grouts and Polymer Modified Mortars PDFDokument7 SeitenStandard Method For Making and Curing Cubes Made From Pre-Bagged Grouts and Polymer Modified Mortars PDFVCNoch keine Bewertungen
- Maths Formula Class10Dokument49 SeitenMaths Formula Class10kaustubh patilNoch keine Bewertungen
- 3516BDokument392 Seiten3516Bmuhammad arif95% (22)
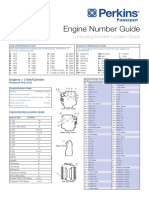
- Engine Number Guide (2-Page)Dokument2 SeitenEngine Number Guide (2-Page)Abdul KhaliqNoch keine Bewertungen
- 1962 Fallout Shelter DesignDokument218 Seiten1962 Fallout Shelter DesignLouie_popwhatski100% (1)
- Design of Timber Roof Truss To British Code - Solved Example - StructvilleDokument9 SeitenDesign of Timber Roof Truss To British Code - Solved Example - StructvilleDeRudy100% (3)
- Science Grade 9: Quarter 4 - Module 6 Heat, Work and EnergyDokument15 SeitenScience Grade 9: Quarter 4 - Module 6 Heat, Work and Energymaesheil computerNoch keine Bewertungen
- Fall Case Log TotalsDokument2 SeitenFall Case Log TotalsBen LemieuxNoch keine Bewertungen
- Qa TableDokument9 SeitenQa Tableapi-295549343Noch keine Bewertungen
- Structsure Report ProneDokument14 SeitenStructsure Report Proneapi-295549343Noch keine Bewertungen
- Evaluation BinderDokument9 SeitenEvaluation Binderapi-295549343Noch keine Bewertungen
- Csi Project Report FinalDokument16 SeitenCsi Project Report Finalapi-295549343Noch keine Bewertungen
- Final Research Paper 2016Dokument16 SeitenFinal Research Paper 2016api-295549343Noch keine Bewertungen
- Total Competency PDFDokument10 SeitenTotal Competency PDFapi-295549343Noch keine Bewertungen
- Topic 2 IgrtDokument3 SeitenTopic 2 Igrtapi-295549343Noch keine Bewertungen
- Professional Service Learning JournalDokument2 SeitenProfessional Service Learning Journalapi-295549343Noch keine Bewertungen
- Spring 2015 Case LogDokument2 SeitenSpring 2015 Case Logapi-280277788Noch keine Bewertungen
- Parotid Clinical Lab Assignment FinalDokument21 SeitenParotid Clinical Lab Assignment Finalapi-295549343Noch keine Bewertungen
- Budget ActivityDokument2 SeitenBudget Activityapi-247490129Noch keine Bewertungen
- Final Competency Semester IIDokument6 SeitenFinal Competency Semester IIapi-295549343Noch keine Bewertungen
- Effective MentoringDokument10 SeitenEffective Mentoringapi-295549343Noch keine Bewertungen
- VagcylDokument7 SeitenVagcylapi-308717184Noch keine Bewertungen
- Lab Planning ProjectDokument10 SeitenLab Planning Projectapi-295549343Noch keine Bewertungen
- Photon CompetenciesDokument2 SeitenPhoton Competenciesapi-295549343Noch keine Bewertungen
- Fall Case Log TotalsDokument2 SeitenFall Case Log TotalsBen LemieuxNoch keine Bewertungen
- Affective Eval SummaryDokument8 SeitenAffective Eval Summaryapi-295549343Noch keine Bewertungen
- Plan Assignment RectumDokument10 SeitenPlan Assignment Rectumapi-295549343Noch keine Bewertungen
- Weekly Discussion 2 10cfr35 SummaryDokument8 SeitenWeekly Discussion 2 10cfr35 Summaryapi-295549343Noch keine Bewertungen
- Case Study FinalDokument11 SeitenCase Study Finalapi-295549343Noch keine Bewertungen
- Leipzig Applicator ConeDokument3 SeitenLeipzig Applicator Coneapi-295549343Noch keine Bewertungen
- Heterogeneity Correction ProjectDokument9 SeitenHeterogeneity Correction Projectapi-295549343100% (1)
- Attenuation ProjectDokument8 SeitenAttenuation Projectapi-295549343Noch keine Bewertungen
- Biological Equivalent DoseDokument3 SeitenBiological Equivalent Doseapi-295549343Noch keine Bewertungen
- Revised Comparative Analysis PaperDokument21 SeitenRevised Comparative Analysis Paperapi-295549343Noch keine Bewertungen
- Ama Challenge 2015Dokument3 SeitenAma Challenge 2015api-295549343Noch keine Bewertungen
- ESD in Fluid Lines: Theory and Application in The Petroleum and Aerospace IndustriesDokument5 SeitenESD in Fluid Lines: Theory and Application in The Petroleum and Aerospace IndustriesKapil DevNoch keine Bewertungen
- Range Gate Generator For FMCW Doppler Raradr PDFDokument5 SeitenRange Gate Generator For FMCW Doppler Raradr PDFSrinivas CherukuNoch keine Bewertungen
- ME101 Lecture08 KD PDFDokument25 SeitenME101 Lecture08 KD PDFR MathewNoch keine Bewertungen
- C-05 April - May-2012Dokument30 SeitenC-05 April - May-2012John SandaNoch keine Bewertungen
- Gazetas 2015 Soil - Footing - Interaction PDFDokument17 SeitenGazetas 2015 Soil - Footing - Interaction PDFMatías MoragaNoch keine Bewertungen
- Speed Control (Switch) - Test 01-03-2010Dokument9 SeitenSpeed Control (Switch) - Test 01-03-2010harikrishnanpd3327Noch keine Bewertungen
- 2008 PJC CH H2 P3 PrelimDokument12 Seiten2008 PJC CH H2 P3 PrelimdeadbeanNoch keine Bewertungen
- Lincolnweld 888 & LA-85Dokument2 SeitenLincolnweld 888 & LA-85Pablo PazNoch keine Bewertungen
- AC O& M City Mall Version 1.0Dokument12 SeitenAC O& M City Mall Version 1.0yewminyun6098Noch keine Bewertungen
- Vib PDFDokument2 SeitenVib PDFprasanna1990Noch keine Bewertungen
- Articulo de Felipe Calizaya (1ra Parte)Dokument5 SeitenArticulo de Felipe Calizaya (1ra Parte)Gustavo PBNoch keine Bewertungen
- ANSA v17.0.0 Release NotesDokument63 SeitenANSA v17.0.0 Release NotesVishnu RaghavanNoch keine Bewertungen
- PEX250í 1200 Instruction ManualDokument10 SeitenPEX250í 1200 Instruction ManualSebastian Aguila RaipanNoch keine Bewertungen
- Task 3 Ronald GarzonDokument23 SeitenTask 3 Ronald GarzonRonal Enrique Garzon SanchezNoch keine Bewertungen
- B SafeunitDokument4 SeitenB SafeunitSabariyantoNoch keine Bewertungen
- Compass SurveyingDokument22 SeitenCompass SurveyingCharles Carpo46% (13)
- A Method of Identifying The Lightning Strike Location On A Structure Hartono ArticleDokument6 SeitenA Method of Identifying The Lightning Strike Location On A Structure Hartono Articlefreddy riveraNoch keine Bewertungen
- Pipesim 2006.1 Fundamentals GasliftDokument13 SeitenPipesim 2006.1 Fundamentals GasliftamulyanaNoch keine Bewertungen
- Laser Ignition For Combustion Engines: January 2004Dokument21 SeitenLaser Ignition For Combustion Engines: January 2004Shekhar ShekharNoch keine Bewertungen
- ECE 6123 Advanced Signal Processing: 1 FiltersDokument9 SeitenECE 6123 Advanced Signal Processing: 1 FiltersJanaki KNoch keine Bewertungen
- English Unit 15Dokument2 SeitenEnglish Unit 15Ruth RodriguezNoch keine Bewertungen
- Hot Plate WeldingDokument2 SeitenHot Plate WeldingsyuepiNoch keine Bewertungen
- Emma Warlinge - Sterilization of Sterile TanksDokument6 SeitenEmma Warlinge - Sterilization of Sterile Tanksaaro_oraalNoch keine Bewertungen