Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Nihms 711050Dokument10 SeitenNihms 711050api-304585193Noch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Babioccheck2009 000Dokument1 SeiteBabioccheck2009 000api-304585193Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- JamesbierdxbetterDokument4 SeitenJamesbierdxbetterapi-304585193100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Paper 1Dokument4 SeitenPaper 1api-304585193Noch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- HW 09Dokument3 SeitenHW 09api-304585193Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Comparative EducationDokument8 SeitenComparative Educationapi-304585193Noch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Homework 920160224192905907-1Dokument8 SeitenHomework 920160224192905907-1api-304585193Noch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Phil of Gender Final PaperDokument8 SeitenPhil of Gender Final Paperapi-304585193Noch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Taylor Deardorff Paper 1 Dna eDokument4 SeitenTaylor Deardorff Paper 1 Dna eapi-304585193Noch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
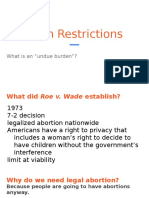
- Abortion Restrictions 1Dokument37 SeitenAbortion Restrictions 1api-304585193Noch keine Bewertungen
- Law 100 Extra CreditDokument9 SeitenLaw 100 Extra Creditapi-304585193Noch keine Bewertungen
- Final Paper Soder Writing Taylor DeardorffDokument10 SeitenFinal Paper Soder Writing Taylor Deardorffapi-304585193Noch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Brandie Conrad counseling infoDokument2 SeitenBrandie Conrad counseling infoMarianLaloNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Punjab Health FoundationDokument29 SeitenPunjab Health FoundationAhsan 11Noch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- CHN QuestionsDokument19 SeitenCHN QuestionsAhlchie C. PiqueroNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Guidehouse - Final ReportDokument68 SeitenGuidehouse - Final ReportGazetteonlineNoch keine Bewertungen
- SSC CR EXAM DETAILSDokument8 SeitenSSC CR EXAM DETAILSkiair kiwoerNoch keine Bewertungen
- Proc No. 177-1999 Registration and Control of ConstructionDokument2 SeitenProc No. 177-1999 Registration and Control of ConstructionTekeba Birhane100% (2)
- SNAP (Food Stamps) : Facts, Myths and RealitiesDokument14 SeitenSNAP (Food Stamps) : Facts, Myths and RealitieshannahNoch keine Bewertungen
- Building State Capability - HarvardDokument276 SeitenBuilding State Capability - HarvardMaajid BashirNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Day 11 PDFDokument16 SeitenDay 11 PDFჯონ ფრაატეეკNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- How Should QuickMedx GrowDokument1 SeiteHow Should QuickMedx Growg14025Noch keine Bewertungen
- Notification UPSC MO Dental Surgeon Other PostsDokument64 SeitenNotification UPSC MO Dental Surgeon Other PostsJeshiNoch keine Bewertungen
- Industrial Action Contingency Plan - West Yorkshire Fire & RescueDokument18 SeitenIndustrial Action Contingency Plan - West Yorkshire Fire & Rescuekhalilv3x6739Noch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Wayne County Community Resource GuideDokument14 SeitenWayne County Community Resource GuideWXYZ-TV Channel 7 DetroitNoch keine Bewertungen
- Supreme Court Rules on Constitutionality of DOH Administrative Order on Breastmilk SubstitutesDokument33 SeitenSupreme Court Rules on Constitutionality of DOH Administrative Order on Breastmilk SubstitutesDaryl CruzNoch keine Bewertungen
- Bloomfield Township Council - Agenda Packet For 11/17/2023Dokument111 SeitenBloomfield Township Council - Agenda Packet For 11/17/2023erickieferNoch keine Bewertungen
- Admission LetterDokument7 SeitenAdmission Letterduke cyberNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Jerry Cochran, Geraldine Cochran v. E.I. Dupont De Nemours, Ren Plastics, Inc., Ciba-Geigy Corporation, American Abrasive Metals Co., Devoe & Raynolds Co., Hoechst Celanese Corporation, Grow Group, Inc., Palmer International, Inc., Jerry Cochran, Geraldine Cochran v. E.I. Dupont De Nemours, Ren Plastics, Inc., Ciba-Geigy Corporation, American Abrasive Metals Co., Devoe & Raynolds Co., Hoechst Celanese Corporation, Grow Group, Inc., Palmer International, Inc., 933 F.2d 1533, 11th Cir. (1991)Dokument12 SeitenJerry Cochran, Geraldine Cochran v. E.I. Dupont De Nemours, Ren Plastics, Inc., Ciba-Geigy Corporation, American Abrasive Metals Co., Devoe & Raynolds Co., Hoechst Celanese Corporation, Grow Group, Inc., Palmer International, Inc., Jerry Cochran, Geraldine Cochran v. E.I. Dupont De Nemours, Ren Plastics, Inc., Ciba-Geigy Corporation, American Abrasive Metals Co., Devoe & Raynolds Co., Hoechst Celanese Corporation, Grow Group, Inc., Palmer International, Inc., 933 F.2d 1533, 11th Cir. (1991)Scribd Government DocsNoch keine Bewertungen
- MSSD PR - Distribution of Assistive Devices To PWDsDokument1 SeiteMSSD PR - Distribution of Assistive Devices To PWDsJonaisa CasanguanNoch keine Bewertungen
- VP Business Development Eclinical Applications in Nashville TN Resume John HedbergDokument2 SeitenVP Business Development Eclinical Applications in Nashville TN Resume John HedbergJohnHedbergNoch keine Bewertungen
- Rules on Judicial Bar Council qualifications for Philippine courtsDokument2 SeitenRules on Judicial Bar Council qualifications for Philippine courtsMLeeNoch keine Bewertungen
- UNT MeningitisprintDokument1 SeiteUNT MeningitisprintPeipur Chakravarthy TejaNoch keine Bewertungen
- Self-Identification of Generic Drug Facilities Sites and Organizations September 2016 Generics GDUFA Self ID Final Guidance2Dokument9 SeitenSelf-Identification of Generic Drug Facilities Sites and Organizations September 2016 Generics GDUFA Self ID Final Guidance2Markbot1999Noch keine Bewertungen
- Maxicare-Affiliated Providers - DOH-Certified Laboratories For COVID-19 Testing As of Sept 29, 2020Dokument2 SeitenMaxicare-Affiliated Providers - DOH-Certified Laboratories For COVID-19 Testing As of Sept 29, 2020Mj BoteroNoch keine Bewertungen
- Iloilo City Regulation Ordinance 2016-084Dokument3 SeitenIloilo City Regulation Ordinance 2016-084Iloilo City CouncilNoch keine Bewertungen
- ISO 22000 Certification Made EasyDokument45 SeitenISO 22000 Certification Made EasymathiarasuNoch keine Bewertungen
- CLEA 2015 (ASIA-INDIA) RespondentsDokument36 SeitenCLEA 2015 (ASIA-INDIA) RespondentsAmol MehtaNoch keine Bewertungen
- Acer Supplier Code of Conduct AuditsDokument6 SeitenAcer Supplier Code of Conduct AuditsshaherikhkhanNoch keine Bewertungen
- Budget PresentationDokument39 SeitenBudget PresentationsajtaurusNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- FORMUL 01796 Lipstick-FormulationDokument2 SeitenFORMUL 01796 Lipstick-FormulationSham Saja100% (1)
- Cases in International LawDokument734 SeitenCases in International LawRbee C. AblanNoch keine Bewertungen