Das könnte Ihnen auch gefallen
- Trump Florida Deposition - 2013Dokument204 SeitenTrump Florida Deposition - 2013Grant Stern100% (1)
- Miami-Dade SMART Transit Plan Report Due Date: August 3rdDokument32 SeitenMiami-Dade SMART Transit Plan Report Due Date: August 3rdGrant SternNoch keine Bewertungen
- Confidential Grounds Lease and Master Development Terms SheetDokument2 SeitenConfidential Grounds Lease and Master Development Terms SheetGrant SternNoch keine Bewertungen
- Richard Tapia - Miami-Dade Elections PRR 8/16/18Dokument6 SeitenRichard Tapia - Miami-Dade Elections PRR 8/16/18Grant SternNoch keine Bewertungen
- Board Conflicts Abound For College Chiefs - The ChronicleDokument6 SeitenBoard Conflicts Abound For College Chiefs - The ChronicleGrant SternNoch keine Bewertungen
- Gennady Klotsman SentencingDokument6 SeitenGennady Klotsman SentencingGrant SternNoch keine Bewertungen
- Trump Capitalizes On Weak U.S. Dollar The CADokument2 SeitenTrump Capitalizes On Weak U.S. Dollar The CAGrant SternNoch keine Bewertungen
- Felix Sater's Cooperation Agreement With The Feds - Salvatore Lauria V Jody Kriss EXHIBIT S 10 1Dokument18 SeitenFelix Sater's Cooperation Agreement With The Feds - Salvatore Lauria V Jody Kriss EXHIBIT S 10 1Grant SternNoch keine Bewertungen
- Mueller Response To Manafort Request To Dismiss VA IndictmentDokument282 SeitenMueller Response To Manafort Request To Dismiss VA IndictmentsonamshethNoch keine Bewertungen
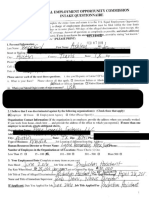
- Ashley Beckford - EEOC Claim vs. InfoWars & Alex JonesDokument25 SeitenAshley Beckford - EEOC Claim vs. InfoWars & Alex JonesGrant Stern100% (1)
- Hitfield ArrabeeDokument12 SeitenHitfield ArrabeeGrant SternNoch keine Bewertungen
- People v. Felix Sater, 201 AD2d 323 (1st of 3) - Criminal AppealDokument35 SeitenPeople v. Felix Sater, 201 AD2d 323 (1st of 3) - Criminal AppealGrant SternNoch keine Bewertungen
- Michael Sater Aka Sheferofsky 2006 Sentencing Hearing TranscriptDokument17 SeitenMichael Sater Aka Sheferofsky 2006 Sentencing Hearing TranscriptGrant Stern100% (1)
- United States of America v. John Doe v. Richard RoeDokument92 SeitenUnited States of America v. John Doe v. Richard RoeGrant Stern100% (1)
- Miami Pine Rocklands Coalition V. Zinke - Ruling On Stay in Favor of DefendantsDokument1 SeiteMiami Pine Rocklands Coalition V. Zinke - Ruling On Stay in Favor of DefendantsGrant SternNoch keine Bewertungen
- Miami Podcast Studios - Final Price SheetDokument1 SeiteMiami Podcast Studios - Final Price SheetGrant SternNoch keine Bewertungen
- House Intel Committee Trump Russia Investigation ReportDokument21 SeitenHouse Intel Committee Trump Russia Investigation ReportGrant Stern100% (3)
- DOJ Letter Warns Nunes Not To Release The Memo Which HE HASN'T EVEN READDokument3 SeitenDOJ Letter Warns Nunes Not To Release The Memo Which HE HASN'T EVEN READGrant Stern100% (1)
- Rick Gates Criminal InformationDokument25 SeitenRick Gates Criminal InformationGrant Stern100% (1)
- Sen. Ron Wyden's Letter To Treasury Secretary Steve MnuchinDokument3 SeitenSen. Ron Wyden's Letter To Treasury Secretary Steve MnuchinPete MaddenNoch keine Bewertungen
- Special Counsel's Office - Internet Research Agency IndictmentDokument37 SeitenSpecial Counsel's Office - Internet Research Agency IndictmentGrant SternNoch keine Bewertungen
- Articles of Incorporation - SoJourn USADokument2 SeitenArticles of Incorporation - SoJourn USAGrant SternNoch keine Bewertungen
- James Michael Hand v. Gov. Rick Scott & State of FloridaDokument43 SeitenJames Michael Hand v. Gov. Rick Scott & State of FloridaGrant Stern100% (1)
- Felix Sater Criminal Docket - Trump SoHo - Unsealing Order, 10-2905Dokument3 SeitenFelix Sater Criminal Docket - Trump SoHo - Unsealing Order, 10-2905Grant Stern80% (5)
- Paul Manafort's Public Relations Strategy MemoDokument1 SeitePaul Manafort's Public Relations Strategy MemoGrant SternNoch keine Bewertungen
- Whistleblower Complaint Against Energy Secretary Rick PerryDokument23 SeitenWhistleblower Complaint Against Energy Secretary Rick PerryGrant SternNoch keine Bewertungen
- Senator Dianne Feinstein (D-CA) Debunks GOP Lies About Russia InvestigationDokument5 SeitenSenator Dianne Feinstein (D-CA) Debunks GOP Lies About Russia InvestigationGrant SternNoch keine Bewertungen
- Sean Spicer Deposition in DNC vs. RNC "Voter Fraud" LawsuitDokument139 SeitenSean Spicer Deposition in DNC vs. RNC "Voter Fraud" LawsuitGrant Stern100% (1)
- Stern vs. Miami II - Case Referred To Special MasterDokument2 SeitenStern vs. Miami II - Case Referred To Special MasterGrant SternNoch keine Bewertungen
- Congressman DeSantis Funded by Trump's Largest DonorsDokument11 SeitenCongressman DeSantis Funded by Trump's Largest DonorsGrant Stern100% (6)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 18-065 State vs. Shaye Marie Bear 5-17-18Dokument47 Seiten18-065 State vs. Shaye Marie Bear 5-17-18JasonTrahanNoch keine Bewertungen
- The History of Valentines Day Text Conversation Topics Dialogs Oneonone Activities Re - 94619Dokument3 SeitenThe History of Valentines Day Text Conversation Topics Dialogs Oneonone Activities Re - 94619mateszylyNoch keine Bewertungen
- Charles DickensDokument12 SeitenCharles DickensLiano NguyễnNoch keine Bewertungen
- Words and Their Characteristics Word Classes: Horse-SDokument2 SeitenWords and Their Characteristics Word Classes: Horse-SsammiedearbornNoch keine Bewertungen
- Dale Anderson Telesford, A079 020 706 (BIA May 27, 2014)Dokument9 SeitenDale Anderson Telesford, A079 020 706 (BIA May 27, 2014)Immigrant & Refugee Appellate Center, LLCNoch keine Bewertungen
- HIT-165 MargoDokument120 SeitenHIT-165 Margosorin610% (1)
- Outrage by John Sandford and Michele CookDokument32 SeitenOutrage by John Sandford and Michele CookRandom House TeensNoch keine Bewertungen
- Crim Digest Mistake of Fact Praeter IntentionemDokument11 SeitenCrim Digest Mistake of Fact Praeter IntentionemCharlotte SagabaenNoch keine Bewertungen
- Final Research Paper Political ScienceDokument5 SeitenFinal Research Paper Political Scienceapi-317898248Noch keine Bewertungen
- Drug Enforcement in The United States: History, Policy, and TrendsDokument30 SeitenDrug Enforcement in The United States: History, Policy, and Trendsanon_560773646Noch keine Bewertungen
- Public Act 336Dokument4 SeitenPublic Act 336Arielle BreenNoch keine Bewertungen
- Linking Words and Collocations - Refreshment CourseDokument27 SeitenLinking Words and Collocations - Refreshment CourseAdalberto Vieira D. FilhoNoch keine Bewertungen
- Sharon Hanes-Crime and Punishment in America - Primary SourcesDokument277 SeitenSharon Hanes-Crime and Punishment in America - Primary SourcesJamesIgroNoch keine Bewertungen
- Dailynews paper 23-11-2023Dokument28 SeitenDailynews paper 23-11-2023Lasitha MuhandiramgeNoch keine Bewertungen
- Dickens' Autobiographical Elements in David Copperfield'Dokument10 SeitenDickens' Autobiographical Elements in David Copperfield'Taibur RahamanNoch keine Bewertungen
- Sparsh Bail Concept of Bail (AutoRecovered)Dokument44 SeitenSparsh Bail Concept of Bail (AutoRecovered)sukhandeep singh100% (1)
- Sentences Types QuizDokument3 SeitenSentences Types QuizAsiale AlmoceraNoch keine Bewertungen
- Flora Drummond The General - Suffragette - Buried CarradaleDokument2 SeitenFlora Drummond The General - Suffragette - Buried CarradaleKintyre On RecordNoch keine Bewertungen
- Motion To Revive and To Lift WarrantDokument2 SeitenMotion To Revive and To Lift WarrantIsay Lim-BorjaNoch keine Bewertungen
- Linne Industries v. Outdoor Water Solutions - ComplaintDokument31 SeitenLinne Industries v. Outdoor Water Solutions - ComplaintSarah BursteinNoch keine Bewertungen
- Politics For The ImprisonedDokument73 SeitenPolitics For The ImprisonedJimWest69Noch keine Bewertungen
- Writing Business Messages PDFDokument20 SeitenWriting Business Messages PDFValda Nurul Izah50% (2)
- Capital Punishment in The PhilippinesDokument27 SeitenCapital Punishment in The PhilippinesLaine KimNoch keine Bewertungen
- Serial Arsonist Jailed For Setting Fire To Wangaratta Home As Elderly Neighbour Slept Inside - ABC NewsDokument2 SeitenSerial Arsonist Jailed For Setting Fire To Wangaratta Home As Elderly Neighbour Slept Inside - ABC NewsKareem AghaNoch keine Bewertungen
- THE PEOPLE OF THE PHILIPPINES, Plaintiff-Appellee, vs. ARCADIO PUESCA Et AlDokument19 SeitenTHE PEOPLE OF THE PHILIPPINES, Plaintiff-Appellee, vs. ARCADIO PUESCA Et AlkimNoch keine Bewertungen
- Best Practice Handbook (Final Draft) PDFDokument92 SeitenBest Practice Handbook (Final Draft) PDFMd Rafiqul IslamNoch keine Bewertungen
- 06-People v. Monticalvo G.R. No. 193507 January 30, 2013Dokument11 Seiten06-People v. Monticalvo G.R. No. 193507 January 30, 2013Jopan SJNoch keine Bewertungen
- The State of Iowa Resists Anna Richter Motion To Expunge Search Warrant and Review Evidence in ChambersDokument259 SeitenThe State of Iowa Resists Anna Richter Motion To Expunge Search Warrant and Review Evidence in ChambersthesacnewsNoch keine Bewertungen
- San Mateo Daily Journal 05-01-19 EditionDokument28 SeitenSan Mateo Daily Journal 05-01-19 EditionSan Mateo Daily JournalNoch keine Bewertungen
- GRE VocabularyDokument192 SeitenGRE VocabularyJerry He100% (1)