Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Behavioral Conduct FormDokument2 SeitenBehavioral Conduct Formapi-253372141Noch keine Bewertungen
- Kin 4203 Emergency Care PlanDokument2 SeitenKin 4203 Emergency Care Planapi-253372141Noch keine Bewertungen
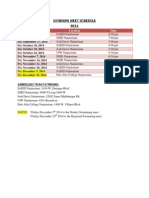
- Swimming Meet ScheduleDokument1 SeiteSwimming Meet Scheduleapi-253372141Noch keine Bewertungen
- Kin 4203 Safety GuidelinesDokument4 SeitenKin 4203 Safety Guidelinesapi-253372141Noch keine Bewertungen
- Track and Field ScheduleDokument1 SeiteTrack and Field Scheduleapi-253372141Noch keine Bewertungen
- Anatomy and Physiology Class ScheduleDokument1 SeiteAnatomy and Physiology Class Scheduleapi-253372141Noch keine Bewertungen
- General Health Class ScheduleDokument1 SeiteGeneral Health Class Scheduleapi-253372141Noch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Kajima-Tiong Seng JV Incident ReportDokument7 SeitenKajima-Tiong Seng JV Incident ReportArjel SagadNoch keine Bewertungen
- Eye Injuries - PosterDokument1 SeiteEye Injuries - PosterMyron CollierNoch keine Bewertungen
- Legal Medicine-Chapter XI & XIXDokument8 SeitenLegal Medicine-Chapter XI & XIXwichupinunoNoch keine Bewertungen
- LMMJ1M Medicolegal Aspects of Physical Injuries 1Dokument7 SeitenLMMJ1M Medicolegal Aspects of Physical Injuries 1Nat HernandezNoch keine Bewertungen
- Introduction To Forensic Science Lecture 5 Forensic PathologyDokument89 SeitenIntroduction To Forensic Science Lecture 5 Forensic PathologyBoţu Alexandru100% (4)
- Homicide disguised as suicide revealed by autopsyDokument3 SeitenHomicide disguised as suicide revealed by autopsyMarlene Gonzalez FcoNoch keine Bewertungen
- Chinese Herbal FormulasDokument8 SeitenChinese Herbal Formulasryandakota100% (1)
- Adult-Onset Subgaleal Hematoma Caused by Hair Pulling: A Rare OccurrenceDokument2 SeitenAdult-Onset Subgaleal Hematoma Caused by Hair Pulling: A Rare OccurrenceAisyah MoslemzzNoch keine Bewertungen
- Case Report: Homicide by A Road Traffic Accident: A Case ReportDokument3 SeitenCase Report: Homicide by A Road Traffic Accident: A Case ReportEdward Arthur IskandarNoch keine Bewertungen
- Muscle and skeleton injuries classificationDokument2 SeitenMuscle and skeleton injuries classificationbf100% (1)
- Emergency Nursing NotesDokument14 SeitenEmergency Nursing NotesJoanne Butac93% (30)
- A Contract Is A Legal AgreementDokument26 SeitenA Contract Is A Legal AgreementalolayaesNoch keine Bewertungen
- Adverse Effects of Fillers and TheirDokument16 SeitenAdverse Effects of Fillers and Theirt3klaNoch keine Bewertungen
- Medical Writing A Police StatementDokument4 SeitenMedical Writing A Police Statementkenc12Noch keine Bewertungen
- Legal MedicineDokument14 SeitenLegal MedicineMinerva Sacar-Guiling91% (56)
- Common Injuries in RecreationDokument17 SeitenCommon Injuries in RecreationRiza Indelible SibullasNoch keine Bewertungen
- Surgery For Cerebral Contusions: Rationale and Practice: Review ArticleDokument4 SeitenSurgery For Cerebral Contusions: Rationale and Practice: Review ArticleIshan SharmaNoch keine Bewertungen
- Contraindications of MassageDokument44 SeitenContraindications of MassageBhargav100% (1)
- Avoid Potato Bruising FINALDokument4 SeitenAvoid Potato Bruising FINALDavid BergotNoch keine Bewertungen
- Patient Assestment PDFDokument12 SeitenPatient Assestment PDFAnonymous 85pLrRNoch keine Bewertungen
- 156.full (1) Badminton InjuriesDokument5 Seiten156.full (1) Badminton InjuriesRaul ValldecabresNoch keine Bewertungen
- Forensic Medicine (Weebly)Dokument7 SeitenForensic Medicine (Weebly)Randal's CaseNoch keine Bewertungen
- Bone Fracture Grp3Dokument12 SeitenBone Fracture Grp3Marjian BaruaNoch keine Bewertungen
- Injury and Overuse Injury.: Classification of Sports InjuriesDokument2 SeitenInjury and Overuse Injury.: Classification of Sports InjuriesVladGrosuNoch keine Bewertungen
- Dressing and BandagesDokument11 SeitenDressing and BandagesNhemia Evangelista ManaloNoch keine Bewertungen
- General PrinciplesDokument61 SeitenGeneral PrinciplesAnda Madalina ZahariaNoch keine Bewertungen
- First Aid LectureDokument36 SeitenFirst Aid LectureRose Anne Riotoc BarrientosNoch keine Bewertungen
- Safety Practices in Sports and ExerciseDokument19 SeitenSafety Practices in Sports and ExerciseRiza Indelible Sibullas80% (5)
- Arrow Wounds and Treatments On The Western FrontierDokument7 SeitenArrow Wounds and Treatments On The Western FrontierbravofNoch keine Bewertungen
- Subconjunctival Hemorrhage OverviewDokument4 SeitenSubconjunctival Hemorrhage OverviewNauli PanjaitanNoch keine Bewertungen