Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Case Report Bacterial MeningitisDokument13 SeitenCase Report Bacterial Meningitisbonziebuddy100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- C Reactive ProteinDokument2 SeitenC Reactive ProteinPorcha PacsayNoch keine Bewertungen
- Freemasonry Uncovering FreemasonryDokument113 SeitenFreemasonry Uncovering Freemasonrycigsas1719100% (1)
- Escherichia E. ColiDokument46 SeitenEscherichia E. ColiInternational Medical Publisher100% (1)
- Principles of Antimicrobial TherapyDokument39 SeitenPrinciples of Antimicrobial TherapyAsthree Nur AzizahNoch keine Bewertungen
- Patient With Fever PDFDokument46 SeitenPatient With Fever PDFNosheen hafeez100% (1)
- Neonatology Clinical Treatment Guidelines OTHER VERSIONDokument94 SeitenNeonatology Clinical Treatment Guidelines OTHER VERSIONAlexandraelsaNoch keine Bewertungen
- Ms Penta NotesDokument84 SeitenMs Penta Notesshenric16Noch keine Bewertungen
- Oman ExamsDokument68 SeitenOman ExamssafasayedNoch keine Bewertungen
- WK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TideDokument43 SeitenWK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TidePotato PceeNoch keine Bewertungen
- Communicable DiseasesDokument20 SeitenCommunicable DiseasesJamaica Manuel Iglesias100% (3)
- Approach To An Unconscious PatientDokument62 SeitenApproach To An Unconscious Patientangiolikkia80% (5)
- Suspected Neurological Conditions Recognition and Referral PDF 66141663923653Dokument76 SeitenSuspected Neurological Conditions Recognition and Referral PDF 66141663923653Alex GasnasNoch keine Bewertungen
- Orofacial Pain - An Update On Diagnosis and Management: PracticeDokument9 SeitenOrofacial Pain - An Update On Diagnosis and Management: PracticeAlex GasnasNoch keine Bewertungen
- Neuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcDokument7 SeitenNeuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcAlex GasnasNoch keine Bewertungen
- Hypoglosal Nerve PalsyDokument4 SeitenHypoglosal Nerve PalsyAlex GasnasNoch keine Bewertungen
- Facial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaDokument6 SeitenFacial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaAlex GasnasNoch keine Bewertungen
- MITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorDokument25 SeitenMITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorAlex GasnasNoch keine Bewertungen
- 2150 FullDokument7 Seiten2150 FullAlex GasnasNoch keine Bewertungen
- Funke Et Al-2011-The Journal of PhysiologyDokument13 SeitenFunke Et Al-2011-The Journal of PhysiologyAlex GasnasNoch keine Bewertungen
- Death PathologyDokument80 SeitenDeath PathologyAlex GasnasNoch keine Bewertungen
- "Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceDokument4 Seiten"Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceAlex GasnasNoch keine Bewertungen
- Post-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraDokument7 SeitenPost-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraAlex GasnasNoch keine Bewertungen
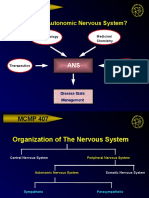
- MCMP 407: Why Study The Autonomic Nervous System?Dokument15 SeitenMCMP 407: Why Study The Autonomic Nervous System?Alex GasnasNoch keine Bewertungen
- CNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaDokument70 SeitenCNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaAlex GasnasNoch keine Bewertungen
- Laboratory Diagnosis of MeningitisDokument28 SeitenLaboratory Diagnosis of Meningitissangeetha_v100Noch keine Bewertungen
- Tuberculous MeningitisDokument34 SeitenTuberculous MeningitisSubchanPrasetyoNoch keine Bewertungen
- Introduction To Expert Systems - MYCINDokument8 SeitenIntroduction To Expert Systems - MYCINVictoria OffomaNoch keine Bewertungen
- Mnemonic SDokument4 SeitenMnemonic S1a2b3c4aNoch keine Bewertungen
- Navarro College Application For AdmissionDokument6 SeitenNavarro College Application For AdmissionNavarro CollegeNoch keine Bewertungen
- Textbook of Diagnostic Microbiology 4th Edition Mahon Test BankDokument13 SeitenTextbook of Diagnostic Microbiology 4th Edition Mahon Test Banklaylafarleyh3i8j9100% (26)
- Micro Bio Disease ListDokument168 SeitenMicro Bio Disease Listspiff spacemanNoch keine Bewertungen
- Complications of OMDokument77 SeitenComplications of OMfahmimiraNoch keine Bewertungen
- Encephalitis and Aseptic Meningitis: Short-Term and Long-Term Outcome, Quality of Life and Neuropsychological FunctioningDokument9 SeitenEncephalitis and Aseptic Meningitis: Short-Term and Long-Term Outcome, Quality of Life and Neuropsychological FunctioningRoberto SoehartonoNoch keine Bewertungen
- Chronic Suppurative Otitis MediaDokument16 SeitenChronic Suppurative Otitis MediaEmil P. MuhammadNoch keine Bewertungen
- Red Flags of The Shoulder and NeckDokument5 SeitenRed Flags of The Shoulder and NecksugoimanNoch keine Bewertungen
- Dr. G. M. Taori: Curriculum VitaeDokument12 SeitenDr. G. M. Taori: Curriculum Vitaesrajan sahuNoch keine Bewertungen
- Neonatal SepsisDokument51 SeitenNeonatal SepsisAngelo Del VentoNoch keine Bewertungen
- Paeds One Word-1-3Dokument18 SeitenPaeds One Word-1-3Killian SibzNoch keine Bewertungen
- Medical Microbiology Specialist Portfolio V4.2reference Copy 2Dokument137 SeitenMedical Microbiology Specialist Portfolio V4.2reference Copy 2cookiedaniel6Noch keine Bewertungen
- HIV NeurologyDokument78 SeitenHIV NeurologyYidnekachewNoch keine Bewertungen
- BffsDokument60 SeitenBffsdrewantaNoch keine Bewertungen
- JASHC 2022 Abstracts19Dokument177 SeitenJASHC 2022 Abstracts19Rodgers SsenyondoNoch keine Bewertungen
- HYDROCEPHALUSDokument6 SeitenHYDROCEPHALUSErika CadawanNoch keine Bewertungen