Das könnte Ihnen auch gefallen
- ACCP-SCCM Critical Care Pharmacy Prep Course 2017 Vol.2 (PDF) WWW - Medicalbr.tkDokument359 SeitenACCP-SCCM Critical Care Pharmacy Prep Course 2017 Vol.2 (PDF) WWW - Medicalbr.tkRoman Lis50% (2)
- Burdock Root AeroponicDokument8 SeitenBurdock Root AeroponicNelson RiddleNoch keine Bewertungen
- A Comparison of Obstetric Maneuvers For The Acute Management of Shoulder DystociaDokument7 SeitenA Comparison of Obstetric Maneuvers For The Acute Management of Shoulder DystociaNellyn Angela HalimNoch keine Bewertungen
- Excerpt From Treating Trauma-Related DissociationDokument14 SeitenExcerpt From Treating Trauma-Related DissociationNortonMentalHealth100% (3)
- Excerpts From IEEE Standard 510-1983Dokument3 SeitenExcerpts From IEEE Standard 510-1983VitalyNoch keine Bewertungen
- Congestive Heart Failure Pathophysiology Schematic DiagramDokument3 SeitenCongestive Heart Failure Pathophysiology Schematic DiagramJasleen KaurNoch keine Bewertungen
- CFSS Monitoring Tool 2019Dokument7 SeitenCFSS Monitoring Tool 2019JULIE100% (10)
- The Placenta and Neurodisability 2nd EditionVon EverandThe Placenta and Neurodisability 2nd EditionIan CrockerNoch keine Bewertungen
- Lüscher Colour TestDokument1 SeiteLüscher Colour TestVicente Sebastián Márquez LecarosNoch keine Bewertungen
- OB GYN EmergenciesDokument266 SeitenOB GYN EmergenciesTemesgen EndalewNoch keine Bewertungen
- 3-PHAP vs. Secretary of Health (Domer)Dokument5 Seiten3-PHAP vs. Secretary of Health (Domer)Arnel ManalastasNoch keine Bewertungen
- SBMWSM2016Dokument491 SeitenSBMWSM2016maimaiyeuem123100% (1)
- CP Neon EncepthDokument9 SeitenCP Neon EncepthJuan Carlos HuanacheaNoch keine Bewertungen
- Contemporary Cesarean Delivery Practice in The United StatesDokument17 SeitenContemporary Cesarean Delivery Practice in The United StatesdedypurnamaNoch keine Bewertungen
- Fetal Surgery - The Ochsner Experience With in Utero Spina Bifida RepairDokument6 SeitenFetal Surgery - The Ochsner Experience With in Utero Spina Bifida RepairJusten ThompsonNoch keine Bewertungen
- Articol 1Dokument7 SeitenArticol 1nistor97Noch keine Bewertungen
- Spina Bifida Is The Most Common of Congenital Anomalies of The Central Nervous System That Are Compatible With LifeDokument9 SeitenSpina Bifida Is The Most Common of Congenital Anomalies of The Central Nervous System That Are Compatible With LifeAlvin De LunaNoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument12 SeitenNIH Public Access: Author ManuscriptAndrea SmithNoch keine Bewertungen
- Effects of Osteopathic Manipulative Treatment On Maternal-Fetal Hemodynamics in Third Trimester Pregnant Women: A Prospective StudyDokument16 SeitenEffects of Osteopathic Manipulative Treatment On Maternal-Fetal Hemodynamics in Third Trimester Pregnant Women: A Prospective StudyMaria LuizaNoch keine Bewertungen
- Jurnal ObstetriDokument7 SeitenJurnal ObstetrikoasimutNoch keine Bewertungen
- Shoulder DystociaDokument8 SeitenShoulder DystociaPorfirio MaciasNoch keine Bewertungen
- Royaldystoci Shoulder 2012 (01-09) PDFDokument9 SeitenRoyaldystoci Shoulder 2012 (01-09) PDFpaolaNoch keine Bewertungen
- Bjo12636 PDFDokument9 SeitenBjo12636 PDFLuphly TaluvtaNoch keine Bewertungen
- Practice Bullet In: Shoulder DystociaDokument11 SeitenPractice Bullet In: Shoulder DystociaMely GallardoNoch keine Bewertungen
- HHS Public Access: Management of Clinical Chorioamnionitis: An Evidence-Based ApproachDokument38 SeitenHHS Public Access: Management of Clinical Chorioamnionitis: An Evidence-Based ApproachIdmNoch keine Bewertungen
- Amsterdam Placental WorkshopDokument16 SeitenAmsterdam Placental WorkshopCarlos Andrés Sánchez RuedaNoch keine Bewertungen
- Develop Med Child Neuro - 2019 - Van Der Looven - Risk Factors For Neonatal Brachial Plexus Palsy A Systematic Review andDokument12 SeitenDevelop Med Child Neuro - 2019 - Van Der Looven - Risk Factors For Neonatal Brachial Plexus Palsy A Systematic Review andNeurisse LauraNoch keine Bewertungen
- Evidence-Based Guidelines For The Management of Abnormally Invasive Placenta Recommendations From The International PDFDokument16 SeitenEvidence-Based Guidelines For The Management of Abnormally Invasive Placenta Recommendations From The International PDFErika GuerreroNoch keine Bewertungen
- Current Status of Percutaneous Umbilical Cord Blood Sampling in JapanDokument9 SeitenCurrent Status of Percutaneous Umbilical Cord Blood Sampling in Japandhea novitaNoch keine Bewertungen
- Correlating Birthweight With Neurological Severity of Obstetric Brachial Plexus LesionsDokument6 SeitenCorrelating Birthweight With Neurological Severity of Obstetric Brachial Plexus LesionsGladstone AsadNoch keine Bewertungen
- Mon 2018Dokument7 SeitenMon 2018Nadieda Ayu MarthalitasariNoch keine Bewertungen
- Epidemiology of Brachial Plexus Palsy in NewbornsDokument7 SeitenEpidemiology of Brachial Plexus Palsy in NewbornsMardyana MardinNoch keine Bewertungen
- The Effect of A Mediolateral Episiotomy During Operative Vaginal Delivery On The Risk of Developing Obstetrical Anal Sphincter InjuriesDokument5 SeitenThe Effect of A Mediolateral Episiotomy During Operative Vaginal Delivery On The Risk of Developing Obstetrical Anal Sphincter InjuriesSanni Rizky PutriNoch keine Bewertungen
- Fetal Growth Velocity in Diabetics and The Risk For Shoulder Dystocia: A Case-Control StudyDokument6 SeitenFetal Growth Velocity in Diabetics and The Risk For Shoulder Dystocia: A Case-Control Studyaulia ilmaNoch keine Bewertungen
- National Trends in The Surgical Management of Meckel's DiverticulumDokument4 SeitenNational Trends in The Surgical Management of Meckel's DiverticulumLeokádio BarrosoNoch keine Bewertungen
- 2016 - Increased Risck For Adhesive Capsulitis of The Shoulder After Cervical DiscDokument5 Seiten2016 - Increased Risck For Adhesive Capsulitis of The Shoulder After Cervical DiscLívia PogettiNoch keine Bewertungen
- Fetal Surgery XDokument11 SeitenFetal Surgery XIoannis ValioulisNoch keine Bewertungen
- Murphy2002 Posthaemorrhagic Ventricular DilatationDokument6 SeitenMurphy2002 Posthaemorrhagic Ventricular DilatationModou NianeNoch keine Bewertungen
- Neonatal Mechanical Ventilation Predictors of Mortality and OutcomesDokument8 SeitenNeonatal Mechanical Ventilation Predictors of Mortality and OutcomesAthenaeum Scientific PublishersNoch keine Bewertungen
- Bakker 2012Dokument10 SeitenBakker 2012ieoNoch keine Bewertungen
- NIH Public Access: Neonatal and Maternal Outcomes With Prolonged Second Stage of LaborDokument18 SeitenNIH Public Access: Neonatal and Maternal Outcomes With Prolonged Second Stage of LabornindhazariaNoch keine Bewertungen
- Ada AdaDokument7 SeitenAda AdaAini AzzahraNoch keine Bewertungen
- 1 Sttri 3Dokument6 Seiten1 Sttri 3parkfishyNoch keine Bewertungen
- The Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaDokument8 SeitenThe Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaAndres GallegosNoch keine Bewertungen
- AbruptionDokument13 SeitenAbruptionMauricio Lopez MejiaNoch keine Bewertungen
- (Sici) 1097 0215 (19970529) 71 5 800 Aid Ijc18 3.0Dokument7 Seiten(Sici) 1097 0215 (19970529) 71 5 800 Aid Ijc18 3.0Moh RamliNoch keine Bewertungen
- 216062-Article Text-532414-1-10-20211014Dokument11 Seiten216062-Article Text-532414-1-10-20211014blitzcanoNoch keine Bewertungen
- Risk Factor For Sever Postpartum Hemorrhage A Case Control StudyDokument9 SeitenRisk Factor For Sever Postpartum Hemorrhage A Case Control StudyAhmad SyaukatNoch keine Bewertungen
- Induction of Labor and Risk of Postpartum Hemorrhage in Low Risk ParturientsDokument8 SeitenInduction of Labor and Risk of Postpartum Hemorrhage in Low Risk ParturientsRudolf Fernando WibowoNoch keine Bewertungen
- Episiotomy in USADokument6 SeitenEpisiotomy in USAFrans Nitu Pa'iNoch keine Bewertungen
- Prognostic Factors and Clinical Features in Liveborn Neonates With Hydrops FetalisDokument6 SeitenPrognostic Factors and Clinical Features in Liveborn Neonates With Hydrops FetalisWulan CerankNoch keine Bewertungen
- Jurnal Abrupsio PlasentaDokument13 SeitenJurnal Abrupsio Plasentaperussi pranadiptaNoch keine Bewertungen
- Ijcm 2014071513394601 PDFDokument9 SeitenIjcm 2014071513394601 PDFnurulrezqiaNoch keine Bewertungen
- Hie GoodDokument8 SeitenHie GoodIkhaAnggieeNoch keine Bewertungen
- The Significance of True Knot of The Umbilical Cord in Long-Term Offspring Neurological HealthDokument13 SeitenThe Significance of True Knot of The Umbilical Cord in Long-Term Offspring Neurological HealthSidonia CatalinaNoch keine Bewertungen
- JCM 10 00123Dokument13 SeitenJCM 10 00123Sidonia CatalinaNoch keine Bewertungen
- Singleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalDokument6 SeitenSingleton Term Breech Deliveries in Nulliparous and Multiparous Women: A 5-Year Experience at The University of Miami/Jackson Memorial HospitalSarah SilaenNoch keine Bewertungen
- Aggressive Intervention of Previable Preterm Premature Rupture of MembranesDokument8 SeitenAggressive Intervention of Previable Preterm Premature Rupture of MembranesVanessa Riaño GodoyNoch keine Bewertungen
- Jurnal Asfiksia ArtikelDokument14 SeitenJurnal Asfiksia Artikelnur_betaNoch keine Bewertungen
- Journal Atonia Uteri YuyunDokument6 SeitenJournal Atonia Uteri YuyunMoh RamliNoch keine Bewertungen
- 33873-Article Text-121761-1-10-20170831Dokument6 Seiten33873-Article Text-121761-1-10-20170831AnggaNoch keine Bewertungen
- R. Irvian1Dokument5 SeitenR. Irvian1Ermawati RohanaNoch keine Bewertungen
- Chouinard2019 PDFDokument8 SeitenChouinard2019 PDFanggunNoch keine Bewertungen
- 9 JurnalDokument83 Seiten9 JurnalWanda AndiniNoch keine Bewertungen
- Hum. Reprod.-2005-Farquharson-3008-11Dokument4 SeitenHum. Reprod.-2005-Farquharson-3008-11venkayammaNoch keine Bewertungen
- AbruptionDokument13 SeitenAbruptionAnghelo Aldair Velásquez CarrilloNoch keine Bewertungen
- Obstetric Catastrophes: A Clinical GuideVon EverandObstetric Catastrophes: A Clinical GuideCarlos MontufarNoch keine Bewertungen
- The Brain of the Critically Ill Pregnant WomanVon EverandThe Brain of the Critically Ill Pregnant WomanJavier Perez-FernandezNoch keine Bewertungen
- Shoulder Dystocia and Birth Injury: Prevention and TreatmentVon EverandShoulder Dystocia and Birth Injury: Prevention and TreatmentNoch keine Bewertungen
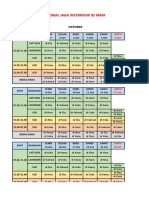
- Jadwal Jaga Internship RS MRMDokument10 SeitenJadwal Jaga Internship RS MRMRahmat AkmalNoch keine Bewertungen
- Bab Iii Kerangka Konsep Dan Definisi OperasionalDokument2 SeitenBab Iii Kerangka Konsep Dan Definisi OperasionalRahmat AkmalNoch keine Bewertungen
- Pengetahuan - 2 Perilaku CrosstabulationDokument4 SeitenPengetahuan - 2 Perilaku CrosstabulationRahmat AkmalNoch keine Bewertungen
- Case Report Ward 23 November 2016Dokument18 SeitenCase Report Ward 23 November 2016Rahmat AkmalNoch keine Bewertungen
- BUNADI, TN - For MergeDokument1 SeiteBUNADI, TN - For MergeRahmat AkmalNoch keine Bewertungen
- Alprazolam PoisoningDokument4 SeitenAlprazolam PoisoningRahmat AkmalNoch keine Bewertungen
- K OnHoukagoLiveTranslationFAQDokument31 SeitenK OnHoukagoLiveTranslationFAQRahmat AkmalNoch keine Bewertungen
- Allergic Rhinitis and Sinusitis inDokument7 SeitenAllergic Rhinitis and Sinusitis inRahmat AkmalNoch keine Bewertungen
- Fatalities Mortal Kombat Vs DC UniverseDokument4 SeitenFatalities Mortal Kombat Vs DC UniverseRahmat AkmalNoch keine Bewertungen
- BM Waste Color CodingDokument23 SeitenBM Waste Color Codingpriyankamote100% (1)
- Pelvic Fracture Case StudyDokument48 SeitenPelvic Fracture Case StudyYves BasanNoch keine Bewertungen
- Bicol Central Academy: Mr. Geo B. AutorDokument4 SeitenBicol Central Academy: Mr. Geo B. AutorGeo AutorNoch keine Bewertungen
- MHFA For SchoolsDokument45 SeitenMHFA For SchoolsLING KUOK LIMNoch keine Bewertungen
- ResumeDokument2 SeitenResumeapi-281248740Noch keine Bewertungen
- Men's Health US - May-June 2023Dokument96 SeitenMen's Health US - May-June 2023albertomnm900Noch keine Bewertungen
- Training 11 Add 3 enDokument44 SeitenTraining 11 Add 3 enBela CruzNoch keine Bewertungen
- Gavi - 2015 Country TA RFIDokument20 SeitenGavi - 2015 Country TA RFIDeepakSinghNoch keine Bewertungen
- Nov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Dokument79 SeitenNov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Jean Gwyneth GatchalianNoch keine Bewertungen
- Preschooler Development by Age and DomainDokument8 SeitenPreschooler Development by Age and DomainThoa KimNoch keine Bewertungen
- Botswana Ref Ranges PaperDokument7 SeitenBotswana Ref Ranges PaperMunyaradzi MangwendezaNoch keine Bewertungen
- Mosh RoomDokument21 SeitenMosh RoomBrandon DishmanNoch keine Bewertungen
- Introduction and Analytical Report PDFDokument111 SeitenIntroduction and Analytical Report PDFJoão Pedro GarciaNoch keine Bewertungen
- Food Data Chart - ZincDokument6 SeitenFood Data Chart - Zinctravi95Noch keine Bewertungen
- Banner AT FM 10k PDFDokument14 SeitenBanner AT FM 10k PDFDamian RamosNoch keine Bewertungen
- Cbse Term 1 Final Exam Instructions 2021-21Dokument9 SeitenCbse Term 1 Final Exam Instructions 2021-21Eshaan123thebestNoch keine Bewertungen
- Jurnal ParuDokument31 SeitenJurnal Parudr. syah sembung wasisoNoch keine Bewertungen
- Job Shadowing PresentationDokument12 SeitenJob Shadowing Presentationapi-462381810Noch keine Bewertungen
- A Beauty 671-680Dokument29 SeitenA Beauty 671-680YollyNoch keine Bewertungen
- IZONE Academic WordlistDokument59 SeitenIZONE Academic WordlistTrung KiênNoch keine Bewertungen
- Tinetti Assessment BalanceDokument2 SeitenTinetti Assessment Balancesathish Lakshmanan100% (1)