Das könnte Ihnen auch gefallen
- Cleft Lip And Palate, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandCleft Lip And Palate, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBewertung: 4.5 von 5 Sternen4.5/5 (3)
- Management of Complications in Oral and Maxillofacial SurgeryVon EverandManagement of Complications in Oral and Maxillofacial SurgeryBewertung: 2 von 5 Sternen2/5 (2)
- Cleft ReviewDokument4 SeitenCleft ReviewAileen Delos Santos-GarciaNoch keine Bewertungen
- Cleft Lip & Palate - KushDokument84 SeitenCleft Lip & Palate - KushKush PathakNoch keine Bewertungen
- Cleft Lip Palate 9801Dokument27 SeitenCleft Lip Palate 9801Achmad HariyantoNoch keine Bewertungen
- Kelompok C PBL 2014Dokument30 SeitenKelompok C PBL 2014Ulfi PutriadiNoch keine Bewertungen
- Periodontal Problems in KidsDokument49 SeitenPeriodontal Problems in KidsRaksmey PhanNoch keine Bewertungen
- Ongoing Debate in Orbital FracturesDokument11 SeitenOngoing Debate in Orbital Fractureslaljadeff12100% (1)
- Normal Occlusion: Presented By: DR Ghulam RasoolDokument41 SeitenNormal Occlusion: Presented By: DR Ghulam RasoolAbdul MohaiminNoch keine Bewertungen
- Non-Caries Dental DiseaseDokument61 SeitenNon-Caries Dental Diseaseapi-19916399Noch keine Bewertungen
- 2020 Tongue Disorders Ods 210Dokument25 Seiten2020 Tongue Disorders Ods 210Farhaana ShaboodienNoch keine Bewertungen
- Role of A Pedodontist in Cleft Lip and Cleft Palate Rehabilitation - An OverviewDokument25 SeitenRole of A Pedodontist in Cleft Lip and Cleft Palate Rehabilitation - An OverviewIJAR JOURNALNoch keine Bewertungen
- Gaint Cell Lesions UPLOADDokument176 SeitenGaint Cell Lesions UPLOADAkshayNoch keine Bewertungen
- Seminar On Cleft Lip: Presented by DR - Cathrine Diana PG IIIDokument93 SeitenSeminar On Cleft Lip: Presented by DR - Cathrine Diana PG IIIcareNoch keine Bewertungen
- Development of Palate: DR - Sowmya K 1 Year PG Dept of ProsthodonticsDokument49 SeitenDevelopment of Palate: DR - Sowmya K 1 Year PG Dept of Prosthodonticssowmya krishnamurthiNoch keine Bewertungen
- Aberrant Frenum and Its TreatmentDokument90 SeitenAberrant Frenum and Its TreatmentheycoolalexNoch keine Bewertungen
- Epidemiology of Oral Cancer PDFDokument6 SeitenEpidemiology of Oral Cancer PDFمحمد عبدالهادي إسماعيلNoch keine Bewertungen
- Developmental Anomalies-DentalDokument16 SeitenDevelopmental Anomalies-DentalMvNoch keine Bewertungen
- Developmental Anamolies of Soft Tissues of Oral CavityDokument73 SeitenDevelopmental Anamolies of Soft Tissues of Oral Cavityvellingiriramesh53040% (1)
- Epidemiologi Dental CariesDokument21 SeitenEpidemiologi Dental CariesSampahAjaNoch keine Bewertungen
- Dev Disturbances of Gingiva and TongueDokument77 SeitenDev Disturbances of Gingiva and TongueNavyy DentNoch keine Bewertungen
- Pit and Fissure SealantsDokument35 SeitenPit and Fissure SealantsshrutiNoch keine Bewertungen
- Potentially Malignant Lesions and ConditionsDokument24 SeitenPotentially Malignant Lesions and ConditionsNaleena Joseph100% (1)
- Periodontal Therapy in Older AdultsDokument15 SeitenPeriodontal Therapy in Older AdultsPathivada Lumbini100% (1)
- Methods of Space Gaining in OrthodonticsDokument41 SeitenMethods of Space Gaining in OrthodonticsAwas AwasNoch keine Bewertungen
- Velopharyngeal IncompetenceDokument14 SeitenVelopharyngeal IncompetenceAzam M Abdullah0% (1)
- Developmental Disturbances of The Oral Mucosa, Gingiva and TongueDokument51 SeitenDevelopmental Disturbances of The Oral Mucosa, Gingiva and Tonguekavin_sandhu100% (1)
- Periodontal DiseasesDokument47 SeitenPeriodontal DiseasesPratikNoch keine Bewertungen
- Management of Open BiteDokument25 SeitenManagement of Open BiteMoola Bharath ReddyNoch keine Bewertungen
- Systemic Diseases Manifested in The JawsDokument25 SeitenSystemic Diseases Manifested in The JawsTeguh Caninus100% (1)
- Khayat - Human Saliva Penetration of Coronally Unsealed Obturated Root Canals-Journal of EndodonticsDokument4 SeitenKhayat - Human Saliva Penetration of Coronally Unsealed Obturated Root Canals-Journal of Endodonticsadioos6767Noch keine Bewertungen
- Cleft Lip& PalateDokument14 SeitenCleft Lip& PalateHusnul Khatimah Imaduddin100% (1)
- Gingival EnlargementDokument125 SeitenGingival Enlargementdr_saurabhsinha_165Noch keine Bewertungen
- Neville's Atlas of Oral Pathology - TEXTODokument488 SeitenNeville's Atlas of Oral Pathology - TEXTOgagandeep singh100% (1)
- School Dental Health Programme PedoDokument37 SeitenSchool Dental Health Programme PedoFourthMolar.comNoch keine Bewertungen
- Dentistry EmergenciesDokument5 SeitenDentistry EmergenciesSofia PereiraNoch keine Bewertungen
- Condylar Fracture & Its ManagementDokument27 SeitenCondylar Fracture & Its Managementriskywhisky100% (1)
- FrenectomyDokument22 SeitenFrenectomyPallav Ganatra100% (3)
- Pulpectomy & ApexificationDokument72 SeitenPulpectomy & ApexificationSimrah AjmalNoch keine Bewertungen
- ANTI-PLAQUE-anticalculus AgentsDokument99 SeitenANTI-PLAQUE-anticalculus Agentst sNoch keine Bewertungen
- Oral Squamous Cell Carcinoma (OSCC)Dokument37 SeitenOral Squamous Cell Carcinoma (OSCC)Yusra Shaukat100% (1)
- ErythroplakiaDokument20 SeitenErythroplakiaEshan VermaNoch keine Bewertungen
- Surgical Management of Oral Pathological LesionDokument24 SeitenSurgical Management of Oral Pathological Lesionمحمد ابوالمجدNoch keine Bewertungen
- CleftlipandpalateDokument134 SeitenCleftlipandpalatePARIJAT CHAKRABORTY100% (1)
- Midface Fractures PART IIDokument64 SeitenMidface Fractures PART IIJomi Porinchu100% (1)
- Detecting Oral CancerDokument2 SeitenDetecting Oral CancerRamon Jose Arandia SarmientoNoch keine Bewertungen
- Cleft Lip and Cleft PalateDokument16 SeitenCleft Lip and Cleft PalateIsmail LubisNoch keine Bewertungen
- Definition:: Types of Forceps Used For Tooth ExtractionDokument28 SeitenDefinition:: Types of Forceps Used For Tooth Extractionayman moaed alyasen100% (1)
- Traumatic Injuries To The Teeth4541Dokument114 SeitenTraumatic Injuries To The Teeth4541Irfan AliNoch keine Bewertungen
- Oral Pre Cancerous LesionsDokument49 SeitenOral Pre Cancerous LesionsAmit MishraNoch keine Bewertungen
- Diseases of Salivary Glands: Prepared By: Dr. Ahlam A. AlesayiDokument96 SeitenDiseases of Salivary Glands: Prepared By: Dr. Ahlam A. AlesayiWaqas Iqbal100% (1)
- Acute Gingival LesionsDokument70 SeitenAcute Gingival LesionsIesha Crawford100% (1)
- Facial Fractures 2Dokument30 SeitenFacial Fractures 2chetotskimdNoch keine Bewertungen
- Mucogingival Surgery (Mucogingival Problems and Management)Dokument46 SeitenMucogingival Surgery (Mucogingival Problems and Management)Dr.Arshad SayedNoch keine Bewertungen
- Controversies in Condylar Fracture Repair UntalanDokument35 SeitenControversies in Condylar Fracture Repair UntalanFrederick Mars Untalan100% (1)
- DiagnosisDokument51 SeitenDiagnosisRamya ChowdaryNoch keine Bewertungen
- AIDS and PeriodontiumDokument25 SeitenAIDS and PeriodontiumKarthik Krishna M100% (1)
- Cleft Lip and Palate Management: A Comprehensive AtlasVon EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNoch keine Bewertungen
- Essential Tissue Healing of the Face and NeckVon EverandEssential Tissue Healing of the Face and NeckBewertung: 5 von 5 Sternen5/5 (2)
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- AnasthesiaDokument2 SeitenAnasthesiaOded KantzukerNoch keine Bewertungen
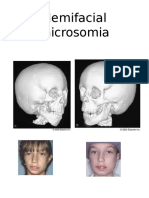
- Hemifacial MicrosomiaDokument2 SeitenHemifacial MicrosomiaOded KantzukerNoch keine Bewertungen
- Composite FillingDokument4 SeitenComposite FillingOded KantzukerNoch keine Bewertungen
- OsteomyelitisofjawDokument35 SeitenOsteomyelitisofjawOded KantzukerNoch keine Bewertungen
- Lec:3 .أ ميهاربا ناحرق لداع.د Principles of tooth preparation 4-Preservation of periodontal tissue:Dokument6 SeitenLec:3 .أ ميهاربا ناحرق لداع.د Principles of tooth preparation 4-Preservation of periodontal tissue:Oded KantzukerNoch keine Bewertungen
- Lec:3 .أ ميهاربا ناحرق لداع.د Principles of tooth preparation 4-Preservation of periodontal tissue:Dokument6 SeitenLec:3 .أ ميهاربا ناحرق لداع.د Principles of tooth preparation 4-Preservation of periodontal tissue:Oded KantzukerNoch keine Bewertungen
- 19-Microendoscopic Lumbar DiscectomyDokument8 Seiten19-Microendoscopic Lumbar DiscectomyNewton IssacNoch keine Bewertungen
- Walt Whitman Video Worksheet. CompletedDokument1 SeiteWalt Whitman Video Worksheet. CompletedelizabethannelangehennigNoch keine Bewertungen
- End of Semester Student SurveyDokument2 SeitenEnd of Semester Student SurveyJoaquinNoch keine Bewertungen
- Allen F. y D. Gale. Comparative Financial SystemsDokument80 SeitenAllen F. y D. Gale. Comparative Financial SystemsCliffordTorresNoch keine Bewertungen
- GooseberriesDokument10 SeitenGooseberriesmoobin.jolfaNoch keine Bewertungen
- Curriculum Vitae: Personal InformationDokument2 SeitenCurriculum Vitae: Personal InformationtyasNoch keine Bewertungen
- Linkedin Job Invite MessageDokument4 SeitenLinkedin Job Invite MessageAxiom IntNoch keine Bewertungen
- Https Emedicine - Medscape.com Article 1831191-PrintDokument59 SeitenHttps Emedicine - Medscape.com Article 1831191-PrintNoviatiPrayangsariNoch keine Bewertungen
- TOURISM AND HOSPITALITY ORGANIZATIONS Di Pa TapooosDokument97 SeitenTOURISM AND HOSPITALITY ORGANIZATIONS Di Pa TapooosDianne EvangelistaNoch keine Bewertungen
- Ikramul (Electrical)Dokument3 SeitenIkramul (Electrical)Ikramu HaqueNoch keine Bewertungen
- Photo Essay (Lyka)Dokument2 SeitenPhoto Essay (Lyka)Lyka LadonNoch keine Bewertungen
- Astm D1895 17Dokument4 SeitenAstm D1895 17Sonia Goncalves100% (1)
- Haloperidol PDFDokument4 SeitenHaloperidol PDFfatimahNoch keine Bewertungen
- Branding Assignment KurkureDokument14 SeitenBranding Assignment KurkureAkriti Jaiswal0% (1)
- SHS StatProb Q4 W1-8 68pgsDokument68 SeitenSHS StatProb Q4 W1-8 68pgsKimberly LoterteNoch keine Bewertungen
- Book Review On PandeymoniumDokument2 SeitenBook Review On PandeymoniumJanhavi ThakkerNoch keine Bewertungen
- E Tech SLHT QTR 2 Week 1Dokument11 SeitenE Tech SLHT QTR 2 Week 1Vie Boldios Roche100% (1)
- DBT Cope Ahead PlanDokument1 SeiteDBT Cope Ahead PlanAmy PowersNoch keine Bewertungen
- Hanumaan Bajrang Baan by JDokument104 SeitenHanumaan Bajrang Baan by JAnonymous R8qkzgNoch keine Bewertungen
- Jesus Chavez AffidavitDokument21 SeitenJesus Chavez AffidavitThe Dallas Morning NewsNoch keine Bewertungen
- 059 Night of The Werewolf PDFDokument172 Seiten059 Night of The Werewolf PDFomar omar100% (1)
- Psychology Research Literature Review ExampleDokument5 SeitenPsychology Research Literature Review Exampleafdtsebxc100% (1)
- English HL P1 Nov 2019Dokument12 SeitenEnglish HL P1 Nov 2019Khathutshelo KharivheNoch keine Bewertungen
- BSBHRM405 Support Recruitment, Selection and Induction of Staff KM2Dokument17 SeitenBSBHRM405 Support Recruitment, Selection and Induction of Staff KM2cplerkNoch keine Bewertungen
- Lifeline® Specialty: Fire Resistant QFCI Cable: Fire Resistant, Flame Retardant Halogen-Free Loose Tube - QFCI/O/RM-JMDokument2 SeitenLifeline® Specialty: Fire Resistant QFCI Cable: Fire Resistant, Flame Retardant Halogen-Free Loose Tube - QFCI/O/RM-JMkevinwz1989Noch keine Bewertungen
- Internal Rules of Procedure Sangguniang BarangayDokument37 SeitenInternal Rules of Procedure Sangguniang Barangayhearty sianenNoch keine Bewertungen
- Improving Downstream Processes To Recover Tartaric AcidDokument10 SeitenImproving Downstream Processes To Recover Tartaric AcidFabio CastellanosNoch keine Bewertungen
- Delegated Legislation in India: Submitted ToDokument15 SeitenDelegated Legislation in India: Submitted ToRuqaiyaNoch keine Bewertungen
- Economics and Agricultural EconomicsDokument28 SeitenEconomics and Agricultural EconomicsM Hossain AliNoch keine Bewertungen
- CS 124/LINGUIST 180 From Languages To Information: Conversational AgentsDokument58 SeitenCS 124/LINGUIST 180 From Languages To Information: Conversational AgentsamanNoch keine Bewertungen