Das könnte Ihnen auch gefallen
- Rule 11DDDokument3 SeitenRule 11DDIonut ColcearNoch keine Bewertungen
- Section 80uDokument3 SeitenSection 80uSukhada SontakkeNoch keine Bewertungen
- Manish Negi A1412020004 Interest Certificate 2015 16Dokument3 SeitenManish Negi A1412020004 Interest Certificate 2015 16Ajinkya Bagade0% (1)
- Self Declaration Form - Sec-80DDokument1 SeiteSelf Declaration Form - Sec-80DDrVarsha Priya SinghNoch keine Bewertungen
- Premium Paid AcknowledgementDokument1 SeitePremium Paid Acknowledgementharsh421Noch keine Bewertungen
- SBI LIFE Premium CertificateDokument1 SeiteSBI LIFE Premium CertificatearithotiNoch keine Bewertungen
- Red Hat Enterprise Linux 8: Upgrading From RHEL 7 To RHEL 8Dokument42 SeitenRed Hat Enterprise Linux 8: Upgrading From RHEL 7 To RHEL 8Richie BallyearsNoch keine Bewertungen
- SBI Insurance 2021Dokument1 SeiteSBI Insurance 2021personal listNoch keine Bewertungen
- Provisional Fy 20-21Dokument1 SeiteProvisional Fy 20-21Kedar YadavNoch keine Bewertungen
- InterestDokument1 SeiteInterestsatya.undapalliNoch keine Bewertungen
- Branch Code:02186 Bank's PAN: Branch Name:: To Whomsoever It May Concern Provisional Home Loan Interest CertificateDokument1 SeiteBranch Code:02186 Bank's PAN: Branch Name:: To Whomsoever It May Concern Provisional Home Loan Interest Certificatesudarsan kingNoch keine Bewertungen
- Duplicate receipt for insurance renewalDokument1 SeiteDuplicate receipt for insurance renewalUTSAV DUBEYNoch keine Bewertungen
- LIC renewal premium receiptDokument1 SeiteLIC renewal premium receiptshivadreamsNoch keine Bewertungen
- Residential home loan EMI and tax deduction detailsDokument1 SeiteResidential home loan EMI and tax deduction detailsXen Operation DPHNoch keine Bewertungen
- CERTIFICATE For Claiming Deduction Under Section 24 (B) & 80C (2) (Xviii) of INCOME TAX ACT, 1961Dokument1 SeiteCERTIFICATE For Claiming Deduction Under Section 24 (B) & 80C (2) (Xviii) of INCOME TAX ACT, 1961Raman SharmaNoch keine Bewertungen
- Sanction LetterDokument3 SeitenSanction Lettern5b859ryf6Noch keine Bewertungen
- Interest Certificate: To Whomsoever It May ConcernDokument1 SeiteInterest Certificate: To Whomsoever It May ConcernfakeNoch keine Bewertungen
- Form No 10-IaDokument1 SeiteForm No 10-IaMd Waseem KNoch keine Bewertungen
- Higher Education Loans BoardDokument8 SeitenHigher Education Loans BoardDON ONNYANGONoch keine Bewertungen
- E Sign DocDokument26 SeitenE Sign DocShaik ShabanaNoch keine Bewertungen
- DonationDokument7 SeitenDonationSwapnil ChodankarNoch keine Bewertungen
- HDFC Ulip 2021-22Dokument2 SeitenHDFC Ulip 2021-22Sandip Kumar Dube100% (1)
- Policy Protection PlanDokument36 SeitenPolicy Protection Plankrishna_1238Noch keine Bewertungen
- Received With Thanks ' 17,967.00 Through Payment Gateway Over The Internet FromDokument1 SeiteReceived With Thanks ' 17,967.00 Through Payment Gateway Over The Internet FromGanesh KumarNoch keine Bewertungen
- Lony3004 00000037809338867 HDokument1 SeiteLony3004 00000037809338867 HlimcysebastinNoch keine Bewertungen
- 524243536624287Dokument1 Seite524243536624287support marenNoch keine Bewertungen
- Tax Declaration Form 2021 22Dokument4 SeitenTax Declaration Form 2021 22Kasiviswanathan ChinnathambiNoch keine Bewertungen
- 80D CertificateDokument2 Seiten80D CertificateSiva KadaliNoch keine Bewertungen
- Sanction Letter For ICICI Bank Car Loan Application of MITESHBHAI SARATANBHAI BHARVAD - NC002047354Dokument1 SeiteSanction Letter For ICICI Bank Car Loan Application of MITESHBHAI SARATANBHAI BHARVAD - NC002047354Sanjay SolankiNoch keine Bewertungen
- ICICI Health InsuranceDokument1 SeiteICICI Health Insurancecanjiatp76260% (1)
- Premium Paid Acknowledgement PDFDokument1 SeitePremium Paid Acknowledgement PDFsanto02Noch keine Bewertungen
- Form No. 10-I: Certificate of Prescribed Authority For The Purposes of Section 80DDBDokument1 SeiteForm No. 10-I: Certificate of Prescribed Authority For The Purposes of Section 80DDBIam KarthikeyanNoch keine Bewertungen
- Lic Premium RecieptDokument1 SeiteLic Premium RecieptGanesh KasleNoch keine Bewertungen
- Home Loan - Certificate - 2022-23Dokument1 SeiteHome Loan - Certificate - 2022-23cont2chandu100% (1)
- Lic PreimumDokument1 SeiteLic PreimumAamir ShahNoch keine Bewertungen
- Name Policy Number Plan Policy Term Premium Paying Term Commencement Date Instalment Premium Mode of Premium Payment Reference CodeDokument1 SeiteName Policy Number Plan Policy Term Premium Paying Term Commencement Date Instalment Premium Mode of Premium Payment Reference CodeVikrant BhaleraoNoch keine Bewertungen
- Education Loan PDFDokument1 SeiteEducation Loan PDFmac martinNoch keine Bewertungen
- NPSPayment ReceiptDokument1 SeiteNPSPayment ReceiptSanthosh DamaNoch keine Bewertungen
- Person With Disability RegistrationDokument2 SeitenPerson With Disability RegistrationSelvakumar KumarNoch keine Bewertungen
- Education Loan PDFDokument7 SeitenEducation Loan PDFSuraj SinghNoch keine Bewertungen
- 1865362Dokument1 Seite1865362Bhavesh ParekhNoch keine Bewertungen
- Loan Ledger - LIC HFL - Customer Portal PDFDokument1 SeiteLoan Ledger - LIC HFL - Customer Portal PDFShisArquamNoch keine Bewertungen
- Received With Thanks ' 2,308.00 Through Payment Gateway Over The Internet FromDokument1 SeiteReceived With Thanks ' 2,308.00 Through Payment Gateway Over The Internet FromKumara RagavendraNoch keine Bewertungen
- Pvss Dav Public School: ReceiptDokument1 SeitePvss Dav Public School: ReceiptSanjeevNoch keine Bewertungen
- Preventive Health Check Up Receipt PDFDokument41 SeitenPreventive Health Check Up Receipt PDFsan mohNoch keine Bewertungen
- Education Loan Interest CertificateDokument1 SeiteEducation Loan Interest CertificatePavan KumarNoch keine Bewertungen
- Renewal Premium Receipt: Har Pal Aapke Sath!!Dokument1 SeiteRenewal Premium Receipt: Har Pal Aapke Sath!!ankit vermaNoch keine Bewertungen
- LIC Aug 2020 PDFDokument1 SeiteLIC Aug 2020 PDFShantanu MetayNoch keine Bewertungen
- Sanction LetterDokument7 SeitenSanction LetterPrimon KarmakarNoch keine Bewertungen
- (AUS) UG Admission Letter 1.2.6Dokument3 Seiten(AUS) UG Admission Letter 1.2.6cheerlife0723Noch keine Bewertungen
- Received With Thanks ' 3,801.00 Through Payment Gateway Over The Internet FromDokument1 SeiteReceived With Thanks ' 3,801.00 Through Payment Gateway Over The Internet FromPratyush 'Jahlad' KunduNoch keine Bewertungen
- Donatekart Foundation: Tax Exempt ReceiptDokument1 SeiteDonatekart Foundation: Tax Exempt ReceiptVishal GandhleNoch keine Bewertungen
- Fertilizer Order GazetteDokument2 SeitenFertilizer Order GazetteUtkarsh ChandelNoch keine Bewertungen
- Section 80-G Donation Receipt CertificateDokument1 SeiteSection 80-G Donation Receipt CertificatePunit MalikNoch keine Bewertungen
- MR Javed Mohammad Monis B295, Chattarpur Enclave, PHASE 2, NEW DELHI-110074Dokument1 SeiteMR Javed Mohammad Monis B295, Chattarpur Enclave, PHASE 2, NEW DELHI-110074javedmonis07Noch keine Bewertungen
- Bank statement for Mr. Radhika Satish MalaniDokument2 SeitenBank statement for Mr. Radhika Satish MalaniVivek ChandakNoch keine Bewertungen
- IntCertEduLoanProvisional10 01 2022Dokument1 SeiteIntCertEduLoanProvisional10 01 2022ajay chaudharyNoch keine Bewertungen
- Prime Minister's National Relief FundDokument1 SeitePrime Minister's National Relief FundindradevhalderNoch keine Bewertungen
- Punjab Maternity Rules SummaryDokument17 SeitenPunjab Maternity Rules SummarySakshi VermaNoch keine Bewertungen
- The Haryana Maternity Benefit RulesDokument19 SeitenThe Haryana Maternity Benefit RulesAdi BahetiNoch keine Bewertungen
- What Is The Difference Between Implicit and Explicit Solutions of The Numerical SolutionsDokument4 SeitenWhat Is The Difference Between Implicit and Explicit Solutions of The Numerical SolutionsnahkbceNoch keine Bewertungen
- The West Bengal School Service CommissionDokument1 SeiteThe West Bengal School Service CommissionnahkbceNoch keine Bewertungen
- 09 Practical Hints Using Numerical Methods Rock MechanicsDokument26 Seiten09 Practical Hints Using Numerical Methods Rock MechanicsnahkbceNoch keine Bewertungen
- Bios ReadmeDokument2 SeitenBios ReadmenahkbceNoch keine Bewertungen
- IIT Kharagpur MTech Student ResumeDokument1 SeiteIIT Kharagpur MTech Student ResumenahkbceNoch keine Bewertungen
- 2BHK Premium Unit Floor Plan with DimensionsDokument1 Seite2BHK Premium Unit Floor Plan with DimensionsnahkbceNoch keine Bewertungen
- DrawDokument1 SeiteDrawnahkbceNoch keine Bewertungen
- Lightweight StructuresDokument6 SeitenLightweight StructureskartikkeyyanNoch keine Bewertungen
- Technical DOUDokument8 SeitenTechnical DOUnahkbceNoch keine Bewertungen
- Appointment RecieptDokument3 SeitenAppointment RecieptnahkbceNoch keine Bewertungen
- PHD Thesis Guidelines IITKGPDokument14 SeitenPHD Thesis Guidelines IITKGPTapojyoti Das50% (2)
- LT Bill Dec16Dokument2 SeitenLT Bill Dec16nahkbceNoch keine Bewertungen
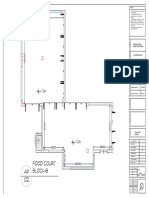
- Aka Food Court Block-BDokument1 SeiteAka Food Court Block-BnahkbceNoch keine Bewertungen
- Esteem Owner's Manual PDFDokument118 SeitenEsteem Owner's Manual PDFnahkbceNoch keine Bewertungen
- SPH Mass ConservationDokument15 SeitenSPH Mass ConservationnahkbceNoch keine Bewertungen
- Subject No-Mi62004, Subject Name-Computational Geomechanics LTP - 3-1-0, CRD - 4Dokument1 SeiteSubject No-Mi62004, Subject Name-Computational Geomechanics LTP - 3-1-0, CRD - 4nahkbceNoch keine Bewertungen
- NT Ed GeDokument1 SeiteNT Ed GenahkbceNoch keine Bewertungen
- 1633 M.B.LiuDokument7 Seiten1633 M.B.LiunahkbceNoch keine Bewertungen
- Conc Form NewDokument5 SeitenConc Form NewnahkbceNoch keine Bewertungen
- ANNmanual 1.1Dokument37 SeitenANNmanual 1.1nahkbceNoch keine Bewertungen
- Structural Drawing 01Dokument1 SeiteStructural Drawing 01nahkbceNoch keine Bewertungen
- Discretisation Techniques For Large Deformation Computational Contact ElastodynamicsDokument236 SeitenDiscretisation Techniques For Large Deformation Computational Contact ElastodynamicsnahkbceNoch keine Bewertungen
- Structural Drawing 03Dokument1 SeiteStructural Drawing 03nahkbceNoch keine Bewertungen
- Kharagpur - Staircase Design PDFDokument38 SeitenKharagpur - Staircase Design PDFjmusopole50% (2)
- Indian Railway Station Code IndexDokument3 SeitenIndian Railway Station Code IndexmayurshahNoch keine Bewertungen
- 2bhk Ordinary Floor PlanDokument1 Seite2bhk Ordinary Floor PlannahkbceNoch keine Bewertungen
- Yield Criteria in 3D PlasticityDokument21 SeitenYield Criteria in 3D Plasticity한종훈100% (1)
- Dynamics - of - Structures Chopra 3rd VersionDokument914 SeitenDynamics - of - Structures Chopra 3rd VersionArsh RaeesNoch keine Bewertungen
- 250 MCQ Front Office Sem VI (NEWDokument41 Seiten250 MCQ Front Office Sem VI (NEWYadnyesh Khot74% (19)
- Guide: ResidenceDokument20 SeitenGuide: ResidenceNicholasFCheongNoch keine Bewertungen
- Sample Travel Consent Letter For ChildrenDokument2 SeitenSample Travel Consent Letter For ChildrenatharkNoch keine Bewertungen
- CS Form No. 212 Personal Data Sheet RevisedDokument4 SeitenCS Form No. 212 Personal Data Sheet RevisedJean Castro76% (106)
- Learn English Podcasts Elementary 01 01 Support Pack TranscriptDokument22 SeitenLearn English Podcasts Elementary 01 01 Support Pack Transcriptpramithbuddika100% (1)
- I-9 Lists of Acceptable DocumentsDokument1 SeiteI-9 Lists of Acceptable Documentskmallon12Noch keine Bewertungen
- Checklist For Tourist Visa PDFDokument3 SeitenChecklist For Tourist Visa PDFTrial MichuNoch keine Bewertungen
- Spain ChecklistDokument2 SeitenSpain ChecklistTouristVisaBookingsNoch keine Bewertungen
- Malaysian Immigration-Checklist For EP (EV)Dokument2 SeitenMalaysian Immigration-Checklist For EP (EV)Rumi AblehNoch keine Bewertungen
- CS Form No. 212 Revised Personal Data Sheet NewDokument4 SeitenCS Form No. 212 Revised Personal Data Sheet Newrhiandy100% (1)
- Basic Passport Checks: Cyan Magenta BlackDokument23 SeitenBasic Passport Checks: Cyan Magenta BlackRakesh KanniNoch keine Bewertungen
- Staff HandbookDokument27 SeitenStaff HandbookRobin RohitNoch keine Bewertungen
- Application PreviewDokument13 SeitenApplication PreviewClient FirstNoch keine Bewertungen
- Oracle HCM Cloud Training Slide 3 - Enhancements OverviewDokument27 SeitenOracle HCM Cloud Training Slide 3 - Enhancements OverviewDhinakaranNoch keine Bewertungen
- Strathfield College Assessment Task 2 Assessment DetailsDokument16 SeitenStrathfield College Assessment Task 2 Assessment DetailsMai NguyễnNoch keine Bewertungen
- Statement of Consent Issuance of A Passport To A MinorDokument1 SeiteStatement of Consent Issuance of A Passport To A MinorHubert PermarNoch keine Bewertungen
- C Visa Englisch Besuch Und Tourismus DataDokument2 SeitenC Visa Englisch Besuch Und Tourismus DataTrailer MojoNoch keine Bewertungen
- Australian Visitor Visa GrantedDokument4 SeitenAustralian Visitor Visa GrantedAlexander BriggsNoch keine Bewertungen
- PolyuDokument21 SeitenPolyuleo666liu666Noch keine Bewertungen
- G.R. No. 169202 March 5, 2010 MARIA VIRGINIA V. REMO, Petitioner,-versus-THE Honorable Secretary of Foreign Affairs, RespondentDokument5 SeitenG.R. No. 169202 March 5, 2010 MARIA VIRGINIA V. REMO, Petitioner,-versus-THE Honorable Secretary of Foreign Affairs, RespondentNadzlah BandilaNoch keine Bewertungen
- Exxon MobilDokument4 SeitenExxon MobilcristinaNoch keine Bewertungen
- Department of Home Affairs DH1738 Form 8Dokument11 SeitenDepartment of Home Affairs DH1738 Form 8Zahidur Ovi RahmanNoch keine Bewertungen
- Blanco Schengenapplicationform - en PDFDokument4 SeitenBlanco Schengenapplicationform - en PDFOlin AllenNoch keine Bewertungen
- UTP PG Admission (Terms & Conditions) - Attachment 1 PDFDokument7 SeitenUTP PG Admission (Terms & Conditions) - Attachment 1 PDFKhaleel HusainNoch keine Bewertungen
- Shafeena CVDokument3 SeitenShafeena CVAbid AliNoch keine Bewertungen
- Italy Tourist ChecklistDokument3 SeitenItaly Tourist ChecklistNitipal SinghNoch keine Bewertungen
- New Zealand Work Permi1Dokument14 SeitenNew Zealand Work Permi1Anonymous pLK3LeBNoch keine Bewertungen
- Step by Step Guide To Getting Turkish Citizenship With InvestmentDokument2 SeitenStep by Step Guide To Getting Turkish Citizenship With InvestmentAshraful Alam MamunNoch keine Bewertungen
- MVV Issue Form (EN) PDFDokument2 SeitenMVV Issue Form (EN) PDFSD W.Noch keine Bewertungen
- Maasai Mara University Kihiu Jane Mwihaki Admission Letter 2019Dokument25 SeitenMaasai Mara University Kihiu Jane Mwihaki Admission Letter 2019Jane mwihakiNoch keine Bewertungen
- The Warmth of Other Suns: The Epic Story of America's Great MigrationVon EverandThe Warmth of Other Suns: The Epic Story of America's Great MigrationBewertung: 4.5 von 5 Sternen4.5/5 (1569)
- You Sound Like a White Girl: The Case for Rejecting AssimilationVon EverandYou Sound Like a White Girl: The Case for Rejecting AssimilationBewertung: 4.5 von 5 Sternen4.5/5 (44)
- LatinoLand: A Portrait of America's Largest and Least Understood MinorityVon EverandLatinoLand: A Portrait of America's Largest and Least Understood MinorityNoch keine Bewertungen
- Reborn in the USA: An Englishman's Love Letter to His Chosen HomeVon EverandReborn in the USA: An Englishman's Love Letter to His Chosen HomeBewertung: 4 von 5 Sternen4/5 (17)
- A Place at the Nayarit: How a Mexican Restaurant Nourished a CommunityVon EverandA Place at the Nayarit: How a Mexican Restaurant Nourished a CommunityNoch keine Bewertungen
- They Came for Freedom: The Forgotten, Epic Adventure of the PilgrimsVon EverandThey Came for Freedom: The Forgotten, Epic Adventure of the PilgrimsBewertung: 4.5 von 5 Sternen4.5/5 (11)
- City of Dreams: The 400-Year Epic History of Immigrant New YorkVon EverandCity of Dreams: The 400-Year Epic History of Immigrant New YorkBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The German Genius: Europe's Third Renaissance, the Second Scientific Revolution, and the Twentieth CenturyVon EverandThe German Genius: Europe's Third Renaissance, the Second Scientific Revolution, and the Twentieth CenturyNoch keine Bewertungen
- Shackled: One Woman’s Dramatic Triumph Over Persecution, Gender Abuse, and a Death SentenceVon EverandShackled: One Woman’s Dramatic Triumph Over Persecution, Gender Abuse, and a Death SentenceBewertung: 5 von 5 Sternen5/5 (17)
- The Long Way Home: An American Journey from Ellis Island to the Great WarVon EverandThe Long Way Home: An American Journey from Ellis Island to the Great WarNoch keine Bewertungen
- Fútbol in the Park: Immigrants, Soccer, and the Creation of Social TiesVon EverandFútbol in the Park: Immigrants, Soccer, and the Creation of Social TiesNoch keine Bewertungen
- We Are Not Refugees: True Stories of the DisplacedVon EverandWe Are Not Refugees: True Stories of the DisplacedBewertung: 4.5 von 5 Sternen4.5/5 (29)
- You Sound Like a White Girl: The Case for Rejecting AssimilationVon EverandYou Sound Like a White Girl: The Case for Rejecting AssimilationNoch keine Bewertungen
- The Hard Road Out: One Woman’s Escape From North KoreaVon EverandThe Hard Road Out: One Woman’s Escape From North KoreaBewertung: 4.5 von 5 Sternen4.5/5 (18)
- Titanic Lives: Migrants and Millionaires, Conmen and CrewVon EverandTitanic Lives: Migrants and Millionaires, Conmen and CrewBewertung: 4 von 5 Sternen4/5 (91)
- Adios, America: The Left's Plan to Turn Our Country into a Third World HellholeVon EverandAdios, America: The Left's Plan to Turn Our Country into a Third World HellholeBewertung: 3.5 von 5 Sternen3.5/5 (35)
- Dear America: Notes of an Undocumented CitizenVon EverandDear America: Notes of an Undocumented CitizenBewertung: 4.5 von 5 Sternen4.5/5 (247)
- The Guarded Gate: Bigotry, Eugenics and the Law That Kept Two Generations of Jews, Italians, and Other European Immigrants Out of AmericaVon EverandThe Guarded Gate: Bigotry, Eugenics and the Law That Kept Two Generations of Jews, Italians, and Other European Immigrants Out of AmericaBewertung: 4.5 von 5 Sternen4.5/5 (43)
- Go Back to Where You Came From: And Other Helpful Recommendations on How to Become an AmericanVon EverandGo Back to Where You Came From: And Other Helpful Recommendations on How to Become an AmericanBewertung: 4.5 von 5 Sternen4.5/5 (14)
- Somewhere We Are Human \ Donde somos humanos (Spanish edition): Historias genuinas sobre migración, sobrevivencia y renaceresVon EverandSomewhere We Are Human \ Donde somos humanos (Spanish edition): Historias genuinas sobre migración, sobrevivencia y renaceresNoch keine Bewertungen
- The Book of Rosy: A Mother’s Story of Separation at the BorderVon EverandThe Book of Rosy: A Mother’s Story of Separation at the BorderBewertung: 4.5 von 5 Sternen4.5/5 (28)
- The Latino Threat: Constructing Immigrants, Citizens, and the Nation, Second EditionVon EverandThe Latino Threat: Constructing Immigrants, Citizens, and the Nation, Second EditionBewertung: 5 von 5 Sternen5/5 (1)
- Dear America: Notes of an Undocumented CitizenVon EverandDear America: Notes of an Undocumented CitizenBewertung: 4.5 von 5 Sternen4.5/5 (106)