Das könnte Ihnen auch gefallen
- BhagavadGita theArtofLeadership OldTextNewContextDokument19 SeitenBhagavadGita theArtofLeadership OldTextNewContextkarmayagnaNoch keine Bewertungen
- Beer Processing PFDDokument1 SeiteBeer Processing PFDkarmayagnaNoch keine Bewertungen
- Borders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudiesDokument22 SeitenBorders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudieskarmayagnaNoch keine Bewertungen
- Spiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerDokument16 SeitenSpiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerkarmayagnaNoch keine Bewertungen
- Logical Flow Diagram of The Production Process OperationsDokument1 SeiteLogical Flow Diagram of The Production Process OperationskarmayagnaNoch keine Bewertungen
- Main Functions of The Operative Manufacturing Execution LevelDokument1 SeiteMain Functions of The Operative Manufacturing Execution LevelkarmayagnaNoch keine Bewertungen
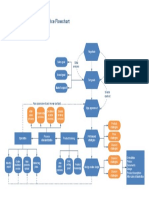
- Ecommerce FlowchartDokument1 SeiteEcommerce FlowchartkarmayagnaNoch keine Bewertungen
- Manufacturing Process MapDokument1 SeiteManufacturing Process MapkarmayagnaNoch keine Bewertungen
- Manufacturing WorkflowDokument1 SeiteManufacturing WorkflowDidik HariadiNoch keine Bewertungen
- Flow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchDokument1 SeiteFlow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchkarmayagnaNoch keine Bewertungen
- Flowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupsDokument1 SeiteFlowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupskarmayagnaNoch keine Bewertungen
- Manufacturing WorkflowDokument1 SeiteManufacturing WorkflowDidik HariadiNoch keine Bewertungen
- Logical Flow Diagram of The Production Process OperationsDokument1 SeiteLogical Flow Diagram of The Production Process OperationskarmayagnaNoch keine Bewertungen
- Manufacturing Process MapDokument1 SeiteManufacturing Process MapkarmayagnaNoch keine Bewertungen
- Logical Flow Diagram of The Production Process OperationsDokument1 SeiteLogical Flow Diagram of The Production Process OperationskarmayagnaNoch keine Bewertungen
- Flowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupsDokument1 SeiteFlowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupskarmayagnaNoch keine Bewertungen
- Services FlowchartDokument1 SeiteServices FlowchartLuis Fernando Sanchez TapiaNoch keine Bewertungen
- Order WorkflowDokument1 SeiteOrder WorkflowkarmayagnaNoch keine Bewertungen
- Order FlowchartDokument1 SeiteOrder FlowchartkarmayagnaNoch keine Bewertungen
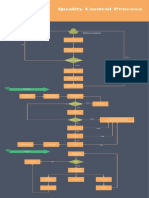
- Quality Control Process: Material SupplierDokument1 SeiteQuality Control Process: Material Supplieralva10 vaNoch keine Bewertungen
- Beer Production ProcessDokument1 SeiteBeer Production ProcesskarmayagnaNoch keine Bewertungen
- Server WorkflowDokument1 SeiteServer WorkflowkarmayagnaNoch keine Bewertungen
- Ecommerce FlowchartDokument1 SeiteEcommerce FlowchartkarmayagnaNoch keine Bewertungen
- Statistical Study For Sonographic Differential Diagnosis ofDokument8 SeitenStatistical Study For Sonographic Differential Diagnosis ofkarmayagnaNoch keine Bewertungen
- Survival After Oral CancerDokument5 SeitenSurvival After Oral CancerkarmayagnaNoch keine Bewertungen
- Oral CancerDokument5 SeitenOral CancerkarmayagnaNoch keine Bewertungen
- Secondary Orbital MlanomasDokument5 SeitenSecondary Orbital MlanomaskarmayagnaNoch keine Bewertungen
- Outcome of SQ .Cell CA of GingivaDokument5 SeitenOutcome of SQ .Cell CA of GingivakarmayagnaNoch keine Bewertungen
- Relationship of Tumor Thickness in Punch Biopsy and SubsequentDokument4 SeitenRelationship of Tumor Thickness in Punch Biopsy and SubsequentkarmayagnaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Scenar CourseDokument29 SeitenScenar Courseretoxproductions100% (7)
- Malaria PDFDokument28 SeitenMalaria PDFKABERA RENENoch keine Bewertungen
- 1-The Etiology of Orthodontic ProblemsDokument47 Seiten1-The Etiology of Orthodontic ProblemsEzza RiezaNoch keine Bewertungen
- Basic AudiologyDokument42 SeitenBasic Audiologyapi-3743483100% (2)
- Case Notes: Requesting Home Care for Robyn HarwoodDokument3 SeitenCase Notes: Requesting Home Care for Robyn Harwoodiduhilag75% (8)
- Layout 2Dokument12 SeitenLayout 2saddam ud dinNoch keine Bewertungen
- DLT211Dokument5 SeitenDLT211Qudus SilmanNoch keine Bewertungen
- Group 1 PWC and Group 2 PWC No Power OptionsDokument3 SeitenGroup 1 PWC and Group 2 PWC No Power OptionslisamaurerNoch keine Bewertungen
- L7 - Induction of LaborDokument8 SeitenL7 - Induction of LaborDheyaa A. SabahNoch keine Bewertungen
- Bodyfensine eDokument2 SeitenBodyfensine eapi-291771056Noch keine Bewertungen
- EDTA IV and Oral Chelation ProtocolDokument10 SeitenEDTA IV and Oral Chelation ProtocolAla MakotaNoch keine Bewertungen
- Blog ConclusionDokument1 SeiteBlog Conclusionapi-240984759Noch keine Bewertungen
- EMS Transfer of Care Form: For Stroke, Chest Pain, Trauma or Altered Mental StatusDokument2 SeitenEMS Transfer of Care Form: For Stroke, Chest Pain, Trauma or Altered Mental StatusAna ManoliuNoch keine Bewertungen
- Access, Continuity & Transition of Care ACT: The General Authority For Healthcare Accreditation & Regulation GaharDokument50 SeitenAccess, Continuity & Transition of Care ACT: The General Authority For Healthcare Accreditation & Regulation GaharElshaimaa AbdelfatahNoch keine Bewertungen
- Code Alert SystemDokument9 SeitenCode Alert SystemSam Tagarda100% (1)
- Virology Sample Questions 1Dokument4 SeitenVirology Sample Questions 1William BufNoch keine Bewertungen
- Kern AttestationDokument120 SeitenKern AttestationBakersfieldNowNoch keine Bewertungen
- Quality of Postnatal Care ServicesDokument10 SeitenQuality of Postnatal Care Servicessaleha sultanaNoch keine Bewertungen
- OPD Form IhealthcareDokument2 SeitenOPD Form IhealthcareSanjay PatilNoch keine Bewertungen
- VRBPAC 12.10.20 Meeting Briefing Document FDADokument53 SeitenVRBPAC 12.10.20 Meeting Briefing Document FDAZerohedge100% (2)
- NMJ Special OncologyDokument24 SeitenNMJ Special OncologyMalcolm LeeNoch keine Bewertungen
- Pedo Revision For Part 1Dokument17 SeitenPedo Revision For Part 1asadNoch keine Bewertungen
- Breastcrawl PDFDokument41 SeitenBreastcrawl PDFFayrouz EssawiNoch keine Bewertungen
- Risk Factors of Anastomotic Leak in Intestinal Surgery AuthorDokument2 SeitenRisk Factors of Anastomotic Leak in Intestinal Surgery AuthorluisNoch keine Bewertungen
- Review On Nature of Inter Display Between Covid 19 and Systemic DiseaseDokument9 SeitenReview On Nature of Inter Display Between Covid 19 and Systemic DiseaseKhalid NNoch keine Bewertungen
- Adv2022 0046Dokument1 SeiteAdv2022 0046Mox LexNoch keine Bewertungen
- Mindsets Matter: A New Framework For Harnessing The Placebo Effect in Modern MedicineDokument24 SeitenMindsets Matter: A New Framework For Harnessing The Placebo Effect in Modern MedicineΑποστολος ΜιχαηλιδηςNoch keine Bewertungen
- Chap 9 The Health Care Delivery SystemDokument26 SeitenChap 9 The Health Care Delivery Systemjocelyn bernardoNoch keine Bewertungen
- Lesson Guide CHN 1RLEDokument8 SeitenLesson Guide CHN 1RLEJonaPhieDomingoMonteroIINoch keine Bewertungen
- Hospital DocumentsDokument17 SeitenHospital DocumentsRaviraj PisheNoch keine Bewertungen