Das könnte Ihnen auch gefallen
- Circuits1 1 Laboratory Meters and Power SupplyDokument2 SeitenCircuits1 1 Laboratory Meters and Power SupplyJad DimabuyuNoch keine Bewertungen
- Heat Transfer by S K Mondal-3-42Dokument40 SeitenHeat Transfer by S K Mondal-3-42Arpit Thakur0% (2)
- Dot 1Dokument5 SeitenDot 1Thomas Nathaniel AngNoch keine Bewertungen
- Assignment 1 - MDDokument3 SeitenAssignment 1 - MDMiguel OcampoNoch keine Bewertungen
- Machine Elements: Cams: Group 7 Charlie Dionisio R - Jhun Lemos Jerphoenix Mullaneda Arsilio SilverioDokument21 SeitenMachine Elements: Cams: Group 7 Charlie Dionisio R - Jhun Lemos Jerphoenix Mullaneda Arsilio SilverioDeniell Joyce MarquezNoch keine Bewertungen
- Me152l - Experiment 5 - AmahmudDokument23 SeitenMe152l - Experiment 5 - AmahmudAli Requiso MahmudNoch keine Bewertungen
- Elements of Energy Systems 2Dokument21 SeitenElements of Energy Systems 2Marcial Jr. MilitanteNoch keine Bewertungen
- Ra 8495 ClarificationsDokument17 SeitenRa 8495 Clarificationsqweqweqweq qweasdqwedqweqwNoch keine Bewertungen
- EE Laws and EthicsDokument17 SeitenEE Laws and Ethicshehe xdNoch keine Bewertungen
- Drop and Hardness Tests of GreasesDokument15 SeitenDrop and Hardness Tests of GreasesGuirigay MarbenJohnNoch keine Bewertungen
- Development of A Reviewer Manual in Mechanical Engineering With Theories and 5,001 Solved Problems and Answered Questions (Elements) : For Computerized Mechanical Engineering Licensure Examination PDFDokument13 SeitenDevelopment of A Reviewer Manual in Mechanical Engineering With Theories and 5,001 Solved Problems and Answered Questions (Elements) : For Computerized Mechanical Engineering Licensure Examination PDFTristan Tabago Consolacion33% (3)
- Power PlantDokument3 SeitenPower PlantVictor John PingkianNoch keine Bewertungen
- Acquired Books Prof ENGG. 2012 2016 RevDokument27 SeitenAcquired Books Prof ENGG. 2012 2016 RevFrei Magsino100% (1)
- Yuri Mechanical Engineers Manual PDFDokument196 SeitenYuri Mechanical Engineers Manual PDFMike Rowen BanaresNoch keine Bewertungen
- Pns Paes 248 2010Dokument18 SeitenPns Paes 248 2010Glaiza Abad FernandezNoch keine Bewertungen
- Board of Mechanical Engineering: Hon. Jesus M. Redelosa, PME, PEE, FPSME, FSPAC, FpameeDokument1 SeiteBoard of Mechanical Engineering: Hon. Jesus M. Redelosa, PME, PEE, FPSME, FSPAC, FpameeBienNoch keine Bewertungen
- Automatic White Board Cleaner ARTICLE 1 DUERRDokument6 SeitenAutomatic White Board Cleaner ARTICLE 1 DUERRborjajovenileNoch keine Bewertungen
- Module 6 Reciprocating COMPRESSORDokument30 SeitenModule 6 Reciprocating COMPRESSORSylvesterNoch keine Bewertungen
- Chapter 1Dokument8 SeitenChapter 1Von A. Damirez0% (1)
- Experiment 1Dokument3 SeitenExperiment 1Ben RileyNoch keine Bewertungen
- Refrigeration-Systems Part 1Dokument11 SeitenRefrigeration-Systems Part 1Sean GuanzonNoch keine Bewertungen
- Handout 3 Types of DC GeneratorsDokument11 SeitenHandout 3 Types of DC GeneratorsAdriel JohnNoch keine Bewertungen
- Chapter II Fluid MachineryDokument90 SeitenChapter II Fluid MachineryFad TajudinNoch keine Bewertungen
- Machine Design 2Dokument255 SeitenMachine Design 2Цедіе Рамос100% (1)
- MCQ in Machine Design and Shop Practice Part 4 ME Board ExamDokument18 SeitenMCQ in Machine Design and Shop Practice Part 4 ME Board ExamKenn Earl Bringino VillanuevaNoch keine Bewertungen
- An Urn Contains 4 Black Balls and 6 White BallsDokument1 SeiteAn Urn Contains 4 Black Balls and 6 White Ballsjc casordNoch keine Bewertungen
- ME463 Plate No. 4 - Anto FINALDokument20 SeitenME463 Plate No. 4 - Anto FINALEman Lampago AntoNoch keine Bewertungen
- Engineering Management WorkDokument51 SeitenEngineering Management WorkPrince El AiunNoch keine Bewertungen
- To Be DownloadDokument2 SeitenTo Be Downloadrex tanong0% (1)
- ME122-1P Cones and Cylinders wk5Dokument12 SeitenME122-1P Cones and Cylinders wk5Llana FroilanNoch keine Bewertungen
- Industrial Plant Engineering Elements Review PDF FreeDokument4 SeitenIndustrial Plant Engineering Elements Review PDF FreeRoss AlteaNoch keine Bewertungen
- HvacDokument20 SeitenHvacJoy CelestialNoch keine Bewertungen
- Fluid-Flow Theory: F MG V GDokument27 SeitenFluid-Flow Theory: F MG V Gcarl domingoNoch keine Bewertungen
- Presentation 1Dokument22 SeitenPresentation 1Cherry ObiasNoch keine Bewertungen
- Review Questions : G(S) C(S)Dokument7 SeitenReview Questions : G(S) C(S)Angel CallejebrioNoch keine Bewertungen
- Powerplant and Industrial Plant Engineering Trial 1: 1 PointsDokument8 SeitenPowerplant and Industrial Plant Engineering Trial 1: 1 PointsJerdNoch keine Bewertungen
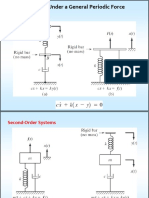
- MEC 410 Chapter 8 Spring 2017Dokument68 SeitenMEC 410 Chapter 8 Spring 2017Frederick KooNoch keine Bewertungen
- First Benchmark PublishingDokument17 SeitenFirst Benchmark PublishingChan Mark AyapanaNoch keine Bewertungen
- Online Lab - Me Lab1 Expt 2 Area MeasurementDokument5 SeitenOnline Lab - Me Lab1 Expt 2 Area MeasurementDessa GuditoNoch keine Bewertungen
- SET A With Answer Key Quiz 2 Fluid Machineries (Prof. Enh. 2)Dokument4 SeitenSET A With Answer Key Quiz 2 Fluid Machineries (Prof. Enh. 2)Famela Gad100% (1)
- Thermodynamics TermsDokument48 SeitenThermodynamics TermsRenniel DingcongNoch keine Bewertungen
- Internal Combustion PDFDokument44 SeitenInternal Combustion PDFMoses DevaprasannaNoch keine Bewertungen
- Descriptive Title: Department of Mechanical EngineeringDokument50 SeitenDescriptive Title: Department of Mechanical EngineeringNikol NekolNoch keine Bewertungen
- Powerplant Reviewer 2Dokument33 SeitenPowerplant Reviewer 2Deyn EstoqueNoch keine Bewertungen
- Module 3 Gears - ClassificationDokument19 SeitenModule 3 Gears - ClassificationBilly JhunNoch keine Bewertungen
- Heat Engine, Pump, RefrigeratorDokument31 SeitenHeat Engine, Pump, RefrigeratorChanna BrarNoch keine Bewertungen
- Me Law, Engineering Ethics and ContractsDokument6 SeitenMe Law, Engineering Ethics and Contractsgoogley71Noch keine Bewertungen
- Top 22 Board Exam Tips You Must Do Right Now by Engr. Adrian CelsoDokument32 SeitenTop 22 Board Exam Tips You Must Do Right Now by Engr. Adrian CelsoIroha IsshikiNoch keine Bewertungen
- Notes DC MACHINES - Compound PDFDokument8 SeitenNotes DC MACHINES - Compound PDFJm PotenciandoNoch keine Bewertungen
- Fluid Machinery Lecture NotesDokument38 SeitenFluid Machinery Lecture NotesMohit KulkarniNoch keine Bewertungen
- MD2Dokument3 SeitenMD2RicaMyrivilleArellagaNoch keine Bewertungen
- CE5620 Intro 2016 8Dokument67 SeitenCE5620 Intro 2016 8Phanendra Kumar AttadaNoch keine Bewertungen
- Ref Systems Lecture Notes 1Dokument9 SeitenRef Systems Lecture Notes 1Retro GamerNoch keine Bewertungen
- Variable Load Problems - KEYDokument1 SeiteVariable Load Problems - KEYChristian M. MortelNoch keine Bewertungen
- PRIME Diagnostic Test 4 MDSP Problem SolvingDokument5 SeitenPRIME Diagnostic Test 4 MDSP Problem SolvingFrankie NovelaNoch keine Bewertungen
- Annex 1 Application Form CHRDR-WaterDokument1 SeiteAnnex 1 Application Form CHRDR-WaterAnonymous ku7POqvKNoch keine Bewertungen
- Supplier QuestionnaireDokument4 SeitenSupplier QuestionnairedorisNoch keine Bewertungen
- Supplier Information SheetDokument2 SeitenSupplier Information SheetJosehermes Santos EstilloreNoch keine Bewertungen
- Professional Electronics Engineer Guidelines For Applicants: Applicant' S ChecklistDokument9 SeitenProfessional Electronics Engineer Guidelines For Applicants: Applicant' S Checklistjj012586Noch keine Bewertungen
- Eteeap Application FormDokument6 SeitenEteeap Application FormsumaychengNoch keine Bewertungen
- G.R. No. 140756 - PEOPLE OF THE PHILIPPINES vs. JUAN GONZALES ESCOTE, ET ALDokument20 SeitenG.R. No. 140756 - PEOPLE OF THE PHILIPPINES vs. JUAN GONZALES ESCOTE, ET ALLucy HeartfiliaNoch keine Bewertungen
- Implementing Value Capture in Latin AmericaDokument72 SeitenImplementing Value Capture in Latin AmericaLincoln Institute of Land PolicyNoch keine Bewertungen
- Sample MCQ II On Negotiable Instruments ActDokument5 SeitenSample MCQ II On Negotiable Instruments ActLokesh RathiNoch keine Bewertungen
- 113761-2002-Lim v. Court of Appeals PDFDokument8 Seiten113761-2002-Lim v. Court of Appeals PDFHans LazaroNoch keine Bewertungen
- For Indiabulls Housing Finance LimitedDokument1 SeiteFor Indiabulls Housing Finance LimitedWild RaacNoch keine Bewertungen
- Document D - Atlanta Constitution-1Dokument2 SeitenDocument D - Atlanta Constitution-1Rafael DevonishNoch keine Bewertungen
- Checklist ISO 14001:2004: (November 2004) Overall Documentation RequirementsDokument5 SeitenChecklist ISO 14001:2004: (November 2004) Overall Documentation RequirementsponggoooNoch keine Bewertungen
- Bir Form 2303Dokument1 SeiteBir Form 2303Maria Sofia OcenarNoch keine Bewertungen
- Perdisco Solution - Transactions - Week 2Dokument11 SeitenPerdisco Solution - Transactions - Week 2My Assignment GuruNoch keine Bewertungen
- Comparative Police SystemDokument52 SeitenComparative Police SystemBong MisalangNoch keine Bewertungen
- (E7) Hearsay (Residual Exception) : Quick RuleDokument112 Seiten(E7) Hearsay (Residual Exception) : Quick Ruleadfsh-1Noch keine Bewertungen
- ERH-Payment Import Format Description BEC-November-2018 - UkDokument15 SeitenERH-Payment Import Format Description BEC-November-2018 - UkCine WorldNoch keine Bewertungen
- Display PDF - PHPDokument21 SeitenDisplay PDF - PHPanshulpatel0608Noch keine Bewertungen
- 4281554Dokument6 Seiten4281554mohitgaba19Noch keine Bewertungen
- Social InequalityDokument2 SeitenSocial InequalityElyza Marie CortezaNoch keine Bewertungen
- NOTES - GOVBUSMAN - Chapters 3 and 4Dokument2 SeitenNOTES - GOVBUSMAN - Chapters 3 and 4Bundalian, Louisse Nicole A.Noch keine Bewertungen
- Complaint Against James McNeile and Andrew Duncan (May 16, 2016)Dokument5 SeitenComplaint Against James McNeile and Andrew Duncan (May 16, 2016)Conflict GateNoch keine Bewertungen
- UnpublishedDokument22 SeitenUnpublishedScribd Government DocsNoch keine Bewertungen
- Civil Aviation Law (En)Dokument25 SeitenCivil Aviation Law (En)vivek kumar guptaNoch keine Bewertungen
- Date/Time Patient PT Status Age SexDokument55 SeitenDate/Time Patient PT Status Age Sexzeerak khanNoch keine Bewertungen
- Financial Action Task ForceDokument10 SeitenFinancial Action Task ForceFaisal HashmiNoch keine Bewertungen
- Tourism Statistics: Kingdom of CambodiaDokument8 SeitenTourism Statistics: Kingdom of CambodiaAubrey LabardaNoch keine Bewertungen
- JDCI Removed PortionsDokument8 SeitenJDCI Removed PortionscriminologyallianceNoch keine Bewertungen
- Motion of Defendant To Plaintiff Produc DocumentsDokument2 SeitenMotion of Defendant To Plaintiff Produc DocumentscjNoch keine Bewertungen
- SST General Male List PDFDokument320 SeitenSST General Male List PDFNoman ShahNoch keine Bewertungen
- Chronology of Important Events Leading To Creation ofDokument27 SeitenChronology of Important Events Leading To Creation ofWaqas MazharNoch keine Bewertungen
- Rule 111Dokument27 SeitenRule 111janbryle.cardenas.21Noch keine Bewertungen
- Mea Member BenefitsDokument14 SeitenMea Member Benefitsapi-84334367Noch keine Bewertungen
- Saili English TranslationDokument2 SeitenSaili English TranslationKaucha WorkNoch keine Bewertungen
- Abbyy® Finereader® 12 SprintDokument12 SeitenAbbyy® Finereader® 12 Sprintoffice komputer3Noch keine Bewertungen