Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Novartis Glivec Case StudyDokument7 SeitenNovartis Glivec Case StudyGarima ParakhNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- MCQ RespiratoryDokument6 SeitenMCQ Respiratorynurulhudaabdulmuiez100% (2)
- A Christian Perspective of Acupuncture: A Research Paper Submitted To DR Keith WarringtonDokument33 SeitenA Christian Perspective of Acupuncture: A Research Paper Submitted To DR Keith WarringtonEric TNoch keine Bewertungen
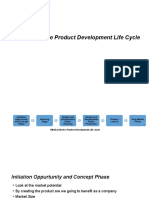
- Medical Device Product Development Life CycleDokument8 SeitenMedical Device Product Development Life CycleSuresh Anand100% (1)
- JSA Form - DemolitionDokument5 SeitenJSA Form - DemolitionARMANINoch keine Bewertungen
- A Real-Time Interactive Augmented Reality Depth Estimation PDFDokument7 SeitenA Real-Time Interactive Augmented Reality Depth Estimation PDFSK sriraamNoch keine Bewertungen
- Template School ProfileDokument4 SeitenTemplate School ProfileCaitlin PeñeraNoch keine Bewertungen
- EWMA Lower Leg Ulcer Diagnosis SuppDokument76 SeitenEWMA Lower Leg Ulcer Diagnosis SuppAna CayumilNoch keine Bewertungen
- Jaspreet Kaur Malerkotla HE Enrolment FormDokument7 SeitenJaspreet Kaur Malerkotla HE Enrolment FormAnmol SinghNoch keine Bewertungen
- Monitoring school safety at block levelDokument4 SeitenMonitoring school safety at block levelSHIVAM KUMARNoch keine Bewertungen
- Zinc Reduces The Detection of Cocaine, Methamphetamine, and THC by ELISA Urine TestingDokument8 SeitenZinc Reduces The Detection of Cocaine, Methamphetamine, and THC by ELISA Urine TestingParvatha SNoch keine Bewertungen
- SolAcne - A Manufacturer of Dermatological Cosmetics Releases Full Anti-Acne Protection Set in EuropeDokument2 SeitenSolAcne - A Manufacturer of Dermatological Cosmetics Releases Full Anti-Acne Protection Set in EuropePR.comNoch keine Bewertungen
- Contact and Contour 2nd SeminarDokument71 SeitenContact and Contour 2nd Seminarrkc456Noch keine Bewertungen
- Highcontainment BiolabsDokument84 SeitenHighcontainment Biolabshansley cookNoch keine Bewertungen
- The Intolerance of Uncertainty Scale: Psychometric Properties of The English VersionDokument15 SeitenThe Intolerance of Uncertainty Scale: Psychometric Properties of The English VersionNoor BahrNoch keine Bewertungen
- CAD-CAM Milled Versus Rapidly Prototyped (3d-Printed) Complete Dentures: An in Vitro Evaluation of TruenessDokument7 SeitenCAD-CAM Milled Versus Rapidly Prototyped (3d-Printed) Complete Dentures: An in Vitro Evaluation of TruenessAkshayaa BalajiNoch keine Bewertungen
- Lockin Specs For Transport VentilatorDokument2 SeitenLockin Specs For Transport VentilatorAlauddin SyahNoch keine Bewertungen
- CPS 2 ToxicologyDokument31 SeitenCPS 2 ToxicologyNgọc Hà NguyễnNoch keine Bewertungen
- Reading For Comprehension 2 SsDokument2 SeitenReading For Comprehension 2 SsJuan Daniel GilNoch keine Bewertungen
- H 046 000181 00 3.0 - DPM4 - Service - ManualDokument88 SeitenH 046 000181 00 3.0 - DPM4 - Service - ManualZeljko TomicNoch keine Bewertungen
- Rapid Smart MethodologyDokument20 SeitenRapid Smart MethodologyOscar Antún Castro HernándezNoch keine Bewertungen
- Global Giving ProposalDokument8 SeitenGlobal Giving ProposalVirnic FarmNoch keine Bewertungen
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDokument18 SeitenWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsMahdi ChahrourNoch keine Bewertungen
- Test BFQDokument13 SeitenTest BFQChristian100% (3)
- DegreeDokument2 SeitenDegreeklraunakNoch keine Bewertungen
- The Salty Kiss (Sample PBL Case)Dokument9 SeitenThe Salty Kiss (Sample PBL Case)c3624343Noch keine Bewertungen
- Brain Health and Nutrition Assessment Form Nutritional Key Assessment Key AE271070116Dokument2 SeitenBrain Health and Nutrition Assessment Form Nutritional Key Assessment Key AE271070116OlesiaNoch keine Bewertungen
- Arch Welding Hazard CHAPTER VDokument4 SeitenArch Welding Hazard CHAPTER VOmengMagcalas100% (1)
- 2016 MACB - Comparison StudyCobas U6500 and U411Dokument1 Seite2016 MACB - Comparison StudyCobas U6500 and U411Dominic EmerencianaNoch keine Bewertungen
- Calculating Pediatric Medication and Fluid DosagesDokument5 SeitenCalculating Pediatric Medication and Fluid DosagesMayank KumarNoch keine Bewertungen