Das könnte Ihnen auch gefallen
- Eye Irrig RDDokument3 SeitenEye Irrig RDJames Kristopher RebayaNoch keine Bewertungen
- Eye IrrigationDokument28 SeitenEye IrrigationAllan NEIGRIHMSNoch keine Bewertungen
- Irrigation of The EyeDokument2 SeitenIrrigation of The EyeissaiahnicolleNoch keine Bewertungen
- NG Tube, Lavage and Gavage Procedure ChecklistDokument6 SeitenNG Tube, Lavage and Gavage Procedure ChecklistBitew Tefera ZewudieNoch keine Bewertungen
- NGT GavageDokument29 SeitenNGT GavageMaan LapitanNoch keine Bewertungen
- Post Op Bed Making ChecklistDokument6 SeitenPost Op Bed Making ChecklistRoselyn Y. QuintoNoch keine Bewertungen
- Tracheostomy CareDokument1 SeiteTracheostomy CareShreyas WalvekarNoch keine Bewertungen
- Care of WoundsDokument6 SeitenCare of WoundsKimpoy Tu-osNoch keine Bewertungen
- Nursing Procedure Checklist: Administering An Ear IrrigationDokument1 SeiteNursing Procedure Checklist: Administering An Ear IrrigationOrl Trinidad0% (1)
- Bed MakingDokument2 SeitenBed Makingtdhaba100% (1)
- Colostomy CareDokument2 SeitenColostomy CareMel RodolfoNoch keine Bewertungen
- Assignment ON MyelographyDokument12 SeitenAssignment ON MyelographyDiana CharaNoch keine Bewertungen
- Wound Care Procedure StudentsDokument2 SeitenWound Care Procedure StudentsJan Philippe BelandoNoch keine Bewertungen
- Umbilical Cord CareDokument11 SeitenUmbilical Cord Carekristel ludangcoNoch keine Bewertungen
- Subcutaneous InjectionDokument2 SeitenSubcutaneous InjectionvishnuNoch keine Bewertungen
- EPILATIONDokument10 SeitenEPILATIONGideon Owusu AttaNoch keine Bewertungen
- POSITIONING CLIENTS IN BED ChecklistDokument2 SeitenPOSITIONING CLIENTS IN BED Checklistbevzie datu100% (1)
- Measuring Body TemperatureDokument5 SeitenMeasuring Body TemperatureJan Jamison ZuluetaNoch keine Bewertungen
- Wound CareDokument3 SeitenWound CaregrangerhermionepNoch keine Bewertungen
- Dilation and Curettage (D&C)Dokument3 SeitenDilation and Curettage (D&C)Jane ElloNoch keine Bewertungen
- Adventist University of The Philippines: Urinary Cathetirization P RIS RemarksDokument2 SeitenAdventist University of The Philippines: Urinary Cathetirization P RIS RemarksAnnie AlbertoNoch keine Bewertungen
- How To Make An Affordable Vein Finder For Use DDokument6 SeitenHow To Make An Affordable Vein Finder For Use DMohammed ShabanNoch keine Bewertungen
- Gloving and Degloving TechniqueDokument23 SeitenGloving and Degloving TechniqueRichard PidlaoanNoch keine Bewertungen
- Establishing and Maintaining A Sterile Field Definition:: Action Rationale Performe D Remarks YES NODokument8 SeitenEstablishing and Maintaining A Sterile Field Definition:: Action Rationale Performe D Remarks YES NOJustin AncogNoch keine Bewertungen
- Nail and Foot CareDokument5 SeitenNail and Foot CareLexie KepnerNoch keine Bewertungen
- Perinal Care FemaleDokument1 SeitePerinal Care FemaleRaquel M. MendozaNoch keine Bewertungen
- Bed BathDokument6 SeitenBed BathLexi LoreNoch keine Bewertungen
- Therapeutic Back Massage: College of NursingDokument1 SeiteTherapeutic Back Massage: College of NursingCarol Neng CalupitanNoch keine Bewertungen
- Nasal Instillation Procedure Guide NursingDokument2 SeitenNasal Instillation Procedure Guide NursingTrisha ApillanesNoch keine Bewertungen
- Checklist For Administrating Inj - Mgso4Dokument3 SeitenChecklist For Administrating Inj - Mgso4Anjali Rahul AjmeriNoch keine Bewertungen
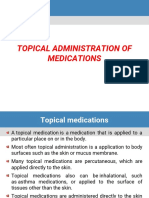
- Instillations and IrrigationsDokument40 SeitenInstillations and IrrigationsAnn Merlin JobinNoch keine Bewertungen
- Tracheostomy CareDokument40 SeitenTracheostomy CareSreelekhaNoch keine Bewertungen
- CHECKLIST - Administering Oral, Sublingual, and Buccal MedicationDokument4 SeitenCHECKLIST - Administering Oral, Sublingual, and Buccal MedicationMichaelNoch keine Bewertungen
- Bedpan or A Urinal: What You Need To Know: What Are Bedpans and Urinals?Dokument8 SeitenBedpan or A Urinal: What You Need To Know: What Are Bedpans and Urinals?Shereen AlobinayNoch keine Bewertungen
- Aceptic Techniques 1Dokument20 SeitenAceptic Techniques 1RimaNoch keine Bewertungen
- Nso ErcpDokument3 SeitenNso Ercptry dokkNoch keine Bewertungen
- Cpms College of Nursing: Assignment ON Colonic IrrigationDokument3 SeitenCpms College of Nursing: Assignment ON Colonic IrrigationAmy Lalringhluani ChhakchhuakNoch keine Bewertungen
- Scrubbing Gloving ChecklistDokument3 SeitenScrubbing Gloving ChecklistLea CelestialNoch keine Bewertungen
- Positioning and Draping The PatientDokument4 SeitenPositioning and Draping The PatientNazire Luis Colita YandugNoch keine Bewertungen
- Linear Arrangements of DR InstrumentsDokument42 SeitenLinear Arrangements of DR Instrumentsxxegyzz100% (1)
- Intramuscular Injection RationaleDokument3 SeitenIntramuscular Injection RationaleDUMMY DUMMYNoch keine Bewertungen
- Bed MakingDokument12 SeitenBed Makingsuman guptaNoch keine Bewertungen
- ) Administering Nasogastric Tube or Orogastric Tube FeedingDokument6 Seiten) Administering Nasogastric Tube or Orogastric Tube FeedingJohn Pearl FernandezNoch keine Bewertungen
- Chapter 7 Giving InjectionDokument21 SeitenChapter 7 Giving InjectionZahwaNoch keine Bewertungen
- FundosDokument13 SeitenFundosLi FaungNoch keine Bewertungen
- Care of Casts and Splints - OrthoInfo - AAOSDokument2 SeitenCare of Casts and Splints - OrthoInfo - AAOSSAIFUL ISLAMNoch keine Bewertungen
- Care of Patients With ColostomyDokument2 SeitenCare of Patients With ColostomysenyorakathNoch keine Bewertungen
- Checklist of IM InjectionDokument5 SeitenChecklist of IM InjectionSharon LawrenceNoch keine Bewertungen
- Immediate Newborn Care GuideDokument8 SeitenImmediate Newborn Care GuideIsabelleNoch keine Bewertungen
- Gastric LavageDokument15 SeitenGastric LavageEm BelandoNoch keine Bewertungen
- Bed MakingDokument5 SeitenBed MakingLea Jean Lobrigo OleaNoch keine Bewertungen
- NGT Feeding: by Group 2Dokument25 SeitenNGT Feeding: by Group 2karl montano100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Cricothyroidotomy and Needle CricothyrotomyDokument10 SeitenCricothyroidotomy and Needle CricothyrotomyDANDYNoch keine Bewertungen
- Eye Irrigation DemoDokument5 SeitenEye Irrigation DemoBabita DhruwNoch keine Bewertungen
- Lumbar Puncture (LP)Dokument10 SeitenLumbar Puncture (LP)Fady Jehad ZabenNoch keine Bewertungen
- Management of Tuberculosis: A guide for clinicians (eBook edition)Von EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Noch keine Bewertungen
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesVon EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNoch keine Bewertungen
- Eye Care With Lesson PlanDokument12 SeitenEye Care With Lesson PlanShekhar Suntha100% (1)
- BIO-Project InvestigatoryDokument83 SeitenBIO-Project InvestigatoryAyush BhattNoch keine Bewertungen
- An Elf and An Orc Had A Little Baby 2Dokument91 SeitenAn Elf and An Orc Had A Little Baby 2alexia alexia100% (2)
- Artificial Salmon SpawningDokument28 SeitenArtificial Salmon SpawningjimborenoNoch keine Bewertungen
- Fairy TaleDokument7 SeitenFairy TaleMiguel Lugia-ZengNoch keine Bewertungen
- MadRiverUnion01 27 21editionDokument10 SeitenMadRiverUnion01 27 21editionMad River UnionNoch keine Bewertungen
- Psychophysiological Detection of Deception Analysis Ii - Course #503Dokument67 SeitenPsychophysiological Detection of Deception Analysis Ii - Course #503John PrasetioNoch keine Bewertungen
- READ: Battle Creek Feral Cats OrdinanceDokument6 SeitenREAD: Battle Creek Feral Cats OrdinanceJennifer BowmanNoch keine Bewertungen
- Animal Diversity 7th Edition Hickman Test Bank 1Dokument9 SeitenAnimal Diversity 7th Edition Hickman Test Bank 1gregoryNoch keine Bewertungen
- Un SMP 2016Dokument27 SeitenUn SMP 2016SmpMugaruNoch keine Bewertungen
- Grade5 Unit1Dokument5 SeitenGrade5 Unit1api-239494748Noch keine Bewertungen
- Gameshark Pokemon GbaDokument76 SeitenGameshark Pokemon Gbanine starNoch keine Bewertungen
- 5th Grade Basic Skills Reading Comprehension and Skills PDFDokument49 Seiten5th Grade Basic Skills Reading Comprehension and Skills PDFAugusto Castellano100% (4)
- Pulpal Reactions To Caries and Dental ProceduresDokument58 SeitenPulpal Reactions To Caries and Dental ProceduresSony RajbhandariNoch keine Bewertungen
- Deteksi Seksual Dimorfisme Pada Benih Ikan Tawes (Barbomymus Gonionotus Bleeker, 1850) Berdasarkan Morfologi Dan AnatomiDokument13 SeitenDeteksi Seksual Dimorfisme Pada Benih Ikan Tawes (Barbomymus Gonionotus Bleeker, 1850) Berdasarkan Morfologi Dan AnatomiSiwiana Dinar UtaminingtyasNoch keine Bewertungen
- The Five Human SensesDokument17 SeitenThe Five Human SensesAntonio Gonzalez100% (1)
- Generic Dungeon WOTCDokument9 SeitenGeneric Dungeon WOTCMark YfjNoch keine Bewertungen
- ?weebee Beginners Bunny CALDokument17 Seiten?weebee Beginners Bunny CALyovanna ortizNoch keine Bewertungen
- About Us: Vaccination AND Deworming ProgramDokument1 SeiteAbout Us: Vaccination AND Deworming ProgramTolitzjr CatayloNoch keine Bewertungen
- Soal SD Kelas 6 Semester 1Dokument13 SeitenSoal SD Kelas 6 Semester 1fadli yasyaNoch keine Bewertungen
- DR Mushtaq Amna Ashraf Aqsa Bashir Ayesha Bibi Hira Nisar Iqra HabibDokument5 SeitenDR Mushtaq Amna Ashraf Aqsa Bashir Ayesha Bibi Hira Nisar Iqra HabibtaibiNoch keine Bewertungen
- Smithsonian Siyc Fall06Dokument16 SeitenSmithsonian Siyc Fall06WilsonHunt100% (1)
- Harcourt GK Phonics Practice Book StudentDokument144 SeitenHarcourt GK Phonics Practice Book StudentІрина КрупаNoch keine Bewertungen
- OSCE - Chest PainDokument2 SeitenOSCE - Chest PaincgalongNoch keine Bewertungen
- Three Faces of Hecate - Ritual PDFDokument3 SeitenThree Faces of Hecate - Ritual PDFEric TuckerNoch keine Bewertungen
- FOM STUDY GUIDE 3rd Block 1Dokument3 SeitenFOM STUDY GUIDE 3rd Block 1Bernadine Cruz Par100% (1)
- Wet & Wild by David EllisDokument83 SeitenWet & Wild by David EllisAustin Macauley Publishers Ltd.Noch keine Bewertungen
- Popcorn Lamb Amigurumi Crochet PDF Free PatternDokument7 SeitenPopcorn Lamb Amigurumi Crochet PDF Free Patternami arinta100% (1)
- Animal Extinction Quiz QuestionsDokument7 SeitenAnimal Extinction Quiz QuestionsHiruna SandeepaNoch keine Bewertungen
- MahitiDokument136 SeitenMahitiSandeep RajvamshyNoch keine Bewertungen
- Basic Anatomy and Physiology of Brain and Spinal CordDokument59 SeitenBasic Anatomy and Physiology of Brain and Spinal CorddrmalikarifNoch keine Bewertungen
- Harry PotterDokument9 SeitenHarry PotterRiaan RaoNoch keine Bewertungen