Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Tongue in Complete DentureDokument8 SeitenTongue in Complete DentureAman SachdevaNoch keine Bewertungen
- Biology ProjectDokument12 SeitenBiology Projectapi-380313126100% (2)
- Narrative Report On School Nursing - EditedDokument16 SeitenNarrative Report On School Nursing - EditedAbby_Cacho_9151100% (2)
- Shëndeti Mendor I Fëmijlve Dhe Adoleshentëve Prizren Naim FanajDokument1 SeiteShëndeti Mendor I Fëmijlve Dhe Adoleshentëve Prizren Naim Fanajlulkuqe029Noch keine Bewertungen
- Cervical DiscographyDokument8 SeitenCervical DiscographyYhoga Timur LagaNoch keine Bewertungen
- ORTHOPAEDICS TRAUMADokument33 SeitenORTHOPAEDICS TRAUMARhomizal MazaliNoch keine Bewertungen
- Variable TypesDokument2 SeitenVariable Typesmarmar418Noch keine Bewertungen
- The Genetics of MicrocephalyDokument6 SeitenThe Genetics of MicrocephalyErsya MuslihNoch keine Bewertungen
- Nursing Care Plan PrenatalDokument5 SeitenNursing Care Plan PrenatalKim Galamgam100% (2)
- HypothyroidismDokument2 SeitenHypothyroidismDanteAndreiNoch keine Bewertungen
- MediShield Life: Better Protection for AllDokument20 SeitenMediShield Life: Better Protection for Alljakovach7Noch keine Bewertungen
- Baby Gap: The Surprising Truth About America's Infant-Mortality RateDokument2 SeitenBaby Gap: The Surprising Truth About America's Infant-Mortality RateJoseph AltmannNoch keine Bewertungen
- Antifungal LectureDokument62 SeitenAntifungal LectureVandana TayalNoch keine Bewertungen
- Psychiatry IntroductionDokument26 SeitenPsychiatry IntroductionMunir AhmedNoch keine Bewertungen
- 45-Fetal & Neonatal AsphyxiaDokument35 Seiten45-Fetal & Neonatal Asphyxiadr_asaleh100% (2)
- Principles of Behavior ChangeDokument10 SeitenPrinciples of Behavior ChangeGuillermo ThomasNoch keine Bewertungen
- Distalization of Maxillary Molars Using A Lever Arm and Mini-ImplantDokument10 SeitenDistalization of Maxillary Molars Using A Lever Arm and Mini-ImplantYury Tenorio CahuanaNoch keine Bewertungen
- Demensia PresentasiDokument49 SeitenDemensia PresentasiDebora Putri Fernanda SaragihNoch keine Bewertungen
- Nurse ResumeDokument1 SeiteNurse Resumeapi-400113721Noch keine Bewertungen
- CC.14.01 Pre and Post Operative CareDokument3 SeitenCC.14.01 Pre and Post Operative CareKrupaNoch keine Bewertungen
- PERINATAL PATIENT SAFETY: Management of Oxytocin For Labor Induction and Augmentation MCN, The American Journal of Maternal/Child NursingDokument2 SeitenPERINATAL PATIENT SAFETY: Management of Oxytocin For Labor Induction and Augmentation MCN, The American Journal of Maternal/Child NursingNishaThakuriNoch keine Bewertungen
- Polisitemia SekunderDokument4 SeitenPolisitemia SekunderAldi RafaelNoch keine Bewertungen
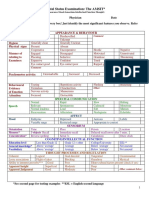
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDokument2 SeitenMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- Asthma Broncial (Theophylline)Dokument41 SeitenAsthma Broncial (Theophylline)Nadya Zahra Henni100% (1)
- Nutrition and Fluid ManagementDokument1 SeiteNutrition and Fluid ManagementCeci NiheNoch keine Bewertungen
- Bone Tumour Synovial Sarcoma Imaging FindingsDokument28 SeitenBone Tumour Synovial Sarcoma Imaging FindingsAnonymous bE4VegCcNoch keine Bewertungen
- Examen Ingles Vocabulario Medico/presente SimpleDokument2 SeitenExamen Ingles Vocabulario Medico/presente SimpleCesarIslasNoch keine Bewertungen
- 2014 AHA/ACC Guidelines for Managing NSTE-ACSDokument46 Seiten2014 AHA/ACC Guidelines for Managing NSTE-ACSEmmieNoch keine Bewertungen
- Tool and Resource Evaluation TemplateDokument4 SeitenTool and Resource Evaluation Templatetimie_reyesNoch keine Bewertungen
- Managing Impaired Gas Exchange and Ineffective Airway ClearanceDokument27 SeitenManaging Impaired Gas Exchange and Ineffective Airway ClearancecuakialyannaNoch keine Bewertungen