Das könnte Ihnen auch gefallen
- Data Integrity and Compliance: A Primer for Medical Product ManufacturersVon EverandData Integrity and Compliance: A Primer for Medical Product ManufacturersNoch keine Bewertungen
- Basic Principles of GMP: GMP For Sterile Pharmaceutical ProductsDokument19 SeitenBasic Principles of GMP: GMP For Sterile Pharmaceutical Productsabhijit_gothoskar6039Noch keine Bewertungen
- IVT Network - Biodecontamination of Cleanrooms and Laboratories Using Gassing Systems - 2017-09-20Dokument13 SeitenIVT Network - Biodecontamination of Cleanrooms and Laboratories Using Gassing Systems - 2017-09-20Le KhoaNoch keine Bewertungen
- Presentation Cleaning ValidationDokument38 SeitenPresentation Cleaning ValidationNishit SuvaNoch keine Bewertungen
- PHSS Annual Members Conference 2014: Book Online Phss - Co.uk/eventsDokument3 SeitenPHSS Annual Members Conference 2014: Book Online Phss - Co.uk/eventsTim SandleNoch keine Bewertungen
- Pharmaceutical Regulatory InspectionsDokument2 SeitenPharmaceutical Regulatory InspectionsTim SandleNoch keine Bewertungen
- 03 VDmax Method1 FAQDokument4 Seiten03 VDmax Method1 FAQFrengki Hadi Eko SantosoNoch keine Bewertungen
- White Paper 10 Problems With Pharma Plant MaintenanceDokument9 SeitenWhite Paper 10 Problems With Pharma Plant MaintenanceAlok Kumar SharmaNoch keine Bewertungen
- Cleaning and Cleaning Validation PDFDokument6 SeitenCleaning and Cleaning Validation PDFedgar palominoNoch keine Bewertungen
- Tim Sandle White Paper EU - GMP - Annex - 1 - The - New - Draft - and - Implications 2020Dokument15 SeitenTim Sandle White Paper EU - GMP - Annex - 1 - The - New - Draft - and - Implications 2020Supriya KapasNoch keine Bewertungen
- GMP Inspections enDokument56 SeitenGMP Inspections ennaokijoe34Noch keine Bewertungen
- Cundell Et Al PDA J Pharm Sci Tech March 2010 (Full Article) SfsDokument21 SeitenCundell Et Al PDA J Pharm Sci Tech March 2010 (Full Article) SfsJessica González LaraNoch keine Bewertungen
- ObjectionableDokument9 SeitenObjectionabledmtalbhogeNoch keine Bewertungen
- Multicenter Study On Incubation Conditions For Environmental Monitoring and Aseptic Process SimulationDokument9 SeitenMulticenter Study On Incubation Conditions For Environmental Monitoring and Aseptic Process SimulationBLUEPRINT Integrated Engineering ServicesNoch keine Bewertungen
- Guidance For Industry - ATP - PremisesDokument13 SeitenGuidance For Industry - ATP - PremisesFISHNoch keine Bewertungen
- Leseprobe FundamentalsDokument14 SeitenLeseprobe FundamentalsDinesh SenathipathiNoch keine Bewertungen
- GMP PartiiDokument76 SeitenGMP PartiiRoger ManzanarezNoch keine Bewertungen
- Retrofitting Existing Lines with RABSDokument28 SeitenRetrofitting Existing Lines with RABSsteven correaNoch keine Bewertungen
- DCVMN Heat Sterilisation v3 1 PDFDokument94 SeitenDCVMN Heat Sterilisation v3 1 PDFmuzammil21_adNoch keine Bewertungen
- White Paper: Preparing For GMP AuditsDokument13 SeitenWhite Paper: Preparing For GMP AuditsDaoNoch keine Bewertungen
- BASIC CYCLE DEVELOPMENT TECHNIQUESDokument7 SeitenBASIC CYCLE DEVELOPMENT TECHNIQUEShasan_j688675Noch keine Bewertungen
- Environmental Monitoring Risk AssessmentDokument22 SeitenEnvironmental Monitoring Risk AssessmentMarcelo CarvalhoNoch keine Bewertungen
- A Final Floor Show For Bugs (Sandle)Dokument4 SeitenA Final Floor Show For Bugs (Sandle)Tim Sandle100% (1)
- Moist Heat SterilizatiojnDokument16 SeitenMoist Heat Sterilizatiojnajitjoshi950Noch keine Bewertungen
- Container Closure Integrity of Sterile Pharmaceutical Containers - Richard MilletDokument36 SeitenContainer Closure Integrity of Sterile Pharmaceutical Containers - Richard MilletmsorianolNoch keine Bewertungen
- An Inside Look at USP71Dokument22 SeitenAn Inside Look at USP71Dante IulliNoch keine Bewertungen
- Cross ContaminationDokument47 SeitenCross ContaminationAKKAD PHARMANoch keine Bewertungen
- USFDA Pharmaceutical GuidelinesDokument5 SeitenUSFDA Pharmaceutical GuidelinesemranNoch keine Bewertungen
- Bioproc PDFDokument6 SeitenBioproc PDFSrijit KhanNoch keine Bewertungen
- WHO IVB 14.07 EngDokument14 SeitenWHO IVB 14.07 EnggineNoch keine Bewertungen
- TunnelDokument2 SeitenTunnelMahesh MahiNoch keine Bewertungen
- Media Simulation TrialsDokument2 SeitenMedia Simulation TrialsTim SandleNoch keine Bewertungen
- Cleaning Sanitisation Disinfection Annex1 PDFDokument4 SeitenCleaning Sanitisation Disinfection Annex1 PDFAbhiNoch keine Bewertungen
- Sampling in Cleaning Validation in Pharmaceutical Industry - Pharmaceutical GuidelinesDokument2 SeitenSampling in Cleaning Validation in Pharmaceutical Industry - Pharmaceutical GuidelinesASHOK KUMAR LENKANoch keine Bewertungen
- IVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Dokument7 SeitenIVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Bhagath VikasNoch keine Bewertungen
- Events Presentations Raci 121126Dokument22 SeitenEvents Presentations Raci 121126mokhtari asmaNoch keine Bewertungen
- 0108 - Change Managament Enabling Quality - Doyle - P10 - FINALDokument14 Seiten0108 - Change Managament Enabling Quality - Doyle - P10 - FINALCesar Rodolfo Angulo DelgadoNoch keine Bewertungen
- PHSSChallenges in Sterile Product ManufacturingDokument4 SeitenPHSSChallenges in Sterile Product ManufacturingTim SandleNoch keine Bewertungen
- PHSS Clarity On GMP Guidance No.3 Qualification of No Touch Transfer For RTU ContainersDokument8 SeitenPHSS Clarity On GMP Guidance No.3 Qualification of No Touch Transfer For RTU ContainersAkuWilliamsNoch keine Bewertungen
- Environmental Control and Measurement: Mark J. StannardDokument42 SeitenEnvironmental Control and Measurement: Mark J. StannardSampada AcharyaNoch keine Bewertungen
- Quality Assurance in Pharma IndustryDokument79 SeitenQuality Assurance in Pharma IndustryMrym NbNoch keine Bewertungen
- 320 Other 1210 2 10 20180111Dokument10 Seiten320 Other 1210 2 10 20180111Vivek PrasadNoch keine Bewertungen
- FDA Warning Letter For Inadequate Batch Record ReviewDokument1 SeiteFDA Warning Letter For Inadequate Batch Record ReviewMina Maher MikhailNoch keine Bewertungen
- Bioburden USP PDFDokument4 SeitenBioburden USP PDFKatyaSNNoch keine Bewertungen
- Disinfectants in Pharmaceutical Industry Tim SandleDokument8 SeitenDisinfectants in Pharmaceutical Industry Tim SandleshwampaNoch keine Bewertungen
- Testing Compressed Air Lines For Microbiological ContaminationDokument8 SeitenTesting Compressed Air Lines For Microbiological Contaminationmuzammil21_adNoch keine Bewertungen
- Guide For Determining The Confidence Interval Using ExcelDokument2 SeitenGuide For Determining The Confidence Interval Using ExcelTim Sandle100% (3)
- Altekar Giacoletti NA17CESEP1 Process Validation Statistical Tool Overvi...Dokument31 SeitenAltekar Giacoletti NA17CESEP1 Process Validation Statistical Tool Overvi...Haroon RasheedNoch keine Bewertungen
- BS Water Treatment Presentation 1 1Dokument44 SeitenBS Water Treatment Presentation 1 1wan yeeNoch keine Bewertungen
- Global Perspectives in Cleaning ValidationDokument17 SeitenGlobal Perspectives in Cleaning ValidationYusuf SalahamanaNoch keine Bewertungen
- Good Documentation Practices - 2014-09-30Dokument1 SeiteGood Documentation Practices - 2014-09-30ApoloTrevinoNoch keine Bewertungen
- Aseptic ProcessingDokument13 SeitenAseptic Processingnsk79in@gmail.comNoch keine Bewertungen
- Who TRS 981 QRMDokument32 SeitenWho TRS 981 QRMrdasarath100% (1)
- Biocontamination Control for Pharmaceuticals and HealthcareVon EverandBiocontamination Control for Pharmaceuticals and HealthcareBewertung: 5 von 5 Sternen5/5 (1)
- Portfolio, Program, and Project Management in the Pharmaceutical and Biotechnology IndustriesVon EverandPortfolio, Program, and Project Management in the Pharmaceutical and Biotechnology IndustriesPete HarpumNoch keine Bewertungen
- Production of Plasma Proteins for Therapeutic UseVon EverandProduction of Plasma Proteins for Therapeutic UseBewertung: 3 von 5 Sternen3/5 (5)
- ICH Quality Guidelines: An Implementation GuideVon EverandICH Quality Guidelines: An Implementation GuideAndrew TeasdaleNoch keine Bewertungen
- Techniques for Downstream process for Biologic Drugs and VaccinesVon EverandTechniques for Downstream process for Biologic Drugs and VaccinesNoch keine Bewertungen
- Comprehensive Quality by Design for Pharmaceutical Product Development and ManufactureVon EverandComprehensive Quality by Design for Pharmaceutical Product Development and ManufactureGintaras V. ReklaitisNoch keine Bewertungen
- Butterfly ValvesDokument3 SeitenButterfly Valvesgepewin2009Noch keine Bewertungen
- 3 TB - Dehumidification and The Psychrometric ChartDokument4 Seiten3 TB - Dehumidification and The Psychrometric Chartashfaq-matte-7993100% (2)
- Article Flow Calculations For Valve SizingDokument13 SeitenArticle Flow Calculations For Valve Sizingashfaq-matte-7993Noch keine Bewertungen
- Valve and Actuator CatalogueDokument60 SeitenValve and Actuator Catalogueashfaq-matte-79930% (1)
- Controls Tips Tricks Manual For FIFA 07 08Dokument6 SeitenControls Tips Tricks Manual For FIFA 07 08ashfaq-matte-7993100% (1)
- Fan SelectionDokument6 SeitenFan Selectionashfaq-matte-7993Noch keine Bewertungen
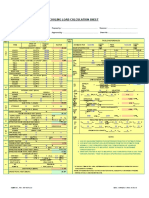
- Cooling Load Calculation Sheet: X X X X X X X X X X X X X X X X Cfm/Person Cfm/DoorDokument6 SeitenCooling Load Calculation Sheet: X X X X X X X X X X X X X X X X Cfm/Person Cfm/Doorashfaq-matte-799375% (4)