Das könnte Ihnen auch gefallen
- Wireless Voice Communication Using LaserDokument2 SeitenWireless Voice Communication Using Laserthiyagar_6100% (4)
- Brain Reading: How National Security Could Gain Access to Our BrainsVon EverandBrain Reading: How National Security Could Gain Access to Our BrainsNoch keine Bewertungen
- Barrie Trower Talks With Victims of Non-Consensual Microwave and EMF Experimentation and Testing - YoutubeDokument9 SeitenBarrie Trower Talks With Victims of Non-Consensual Microwave and EMF Experimentation and Testing - YoutubeEmil-WendtlandNoch keine Bewertungen
- Response of Brain Tissue To Chronically Implanted Neural ElectrodesDokument18 SeitenResponse of Brain Tissue To Chronically Implanted Neural ElectrodesNihal Ahmed MabroukNoch keine Bewertungen
- Case 8:18-cv-01644-VAP-KES Document 74 Filed 04/18/19 Page 1 of 5 Page ID #:2153Dokument5 SeitenCase 8:18-cv-01644-VAP-KES Document 74 Filed 04/18/19 Page 1 of 5 Page ID #:2153EvieM.Warner100% (1)
- Geolocational Privacy and Surveillance (GPS) Act: HearingDokument208 SeitenGeolocational Privacy and Surveillance (GPS) Act: HearingScribd Government Docs100% (1)
- United States v. Bruce Winston, 4th Cir. (2016)Dokument16 SeitenUnited States v. Bruce Winston, 4th Cir. (2016)Scribd Government Docs100% (1)
- GCSB Project CORTEXDokument19 SeitenGCSB Project CORTEXLeakSourceInfo100% (1)
- Remote-Controlled ManDokument2 SeitenRemote-Controlled ManScribdata100% (11)
- US v. Timothy GrahamDokument9 SeitenUS v. Timothy GrahamRussell BrandomNoch keine Bewertungen
- Technical Aspects of Lawful InterceptionDokument12 SeitenTechnical Aspects of Lawful InterceptionITU-T Technology Watch67% (3)
- Adult Neurological QuestionnaireDokument1 SeiteAdult Neurological QuestionnaireIqbal BaryarNoch keine Bewertungen
- Communication Networks Leon Garcia PDF DownloadDokument3 SeitenCommunication Networks Leon Garcia PDF DownloadSudesh Agrawal0% (3)
- Human Rights AlertDokument120 SeitenHuman Rights AlertHuman Rights Alert - NGO (RA)Noch keine Bewertungen
- Case 1:20-cv-02658-CJN Document 60 Filed 12/07/20Dokument35 SeitenCase 1:20-cv-02658-CJN Document 60 Filed 12/07/20The VergeNoch keine Bewertungen
- Free Space Laser CommunicationDokument19 SeitenFree Space Laser CommunicationSourav Sahoo100% (1)
- Strahlenfolter - TI - How To Detect Electronic Harassment Easy - Targeted Individuals - YoutubeDokument44 SeitenStrahlenfolter - TI - How To Detect Electronic Harassment Easy - Targeted Individuals - YoutubeTimo_KaehlkeNoch keine Bewertungen
- U.S. Patent 6,011,991Dokument17 SeitenU.S. Patent 6,011,991ResearchingPubNoch keine Bewertungen
- Ieee Research Paper On Brain Computer InterfaceDokument10 SeitenIeee Research Paper On Brain Computer Interfacefvgy6fn3100% (1)
- Reply To Scott McInerney, Director Executive Investigations, FDLE Jun-28-2019Dokument58 SeitenReply To Scott McInerney, Director Executive Investigations, FDLE Jun-28-2019Neil Gillespie100% (1)
- IMDDokument111 SeitenIMDTwintu VinishNoch keine Bewertungen
- Low Cost Prototype Simulation of Spectrum Analyzer Base On GNU Radio and RTL-SDRDokument13 SeitenLow Cost Prototype Simulation of Spectrum Analyzer Base On GNU Radio and RTL-SDRBambang Bagus HariantoNoch keine Bewertungen
- Artificial Intelligence Based Real-Time Attendance System Using Face RecognitionDokument66 SeitenArtificial Intelligence Based Real-Time Attendance System Using Face RecognitiongururajNoch keine Bewertungen
- Bio Telemetry Final ReportDokument40 SeitenBio Telemetry Final Reportmeghayu_adhvaryuNoch keine Bewertungen
- Personal Data Privacy and Security Act of 2011Dokument70 SeitenPersonal Data Privacy and Security Act of 2011s_klineNoch keine Bewertungen
- Thaens - NATO Cooperative ESM OperationsDokument11 SeitenThaens - NATO Cooperative ESM OperationsMartin Schweighart MoyaNoch keine Bewertungen
- Wrocklage V DHSDokument13 SeitenWrocklage V DHSFedSmith Inc.Noch keine Bewertungen
- GBPPR Active Denial SystemDokument30 SeitenGBPPR Active Denial SystemRobert EckardtNoch keine Bewertungen
- Magic MonitorDokument178 SeitenMagic MonitorAbdul LateefNoch keine Bewertungen
- TOP SECRET NSA Inspector General Report On Email & Internet Data Collection Under Stellar WindDokument51 SeitenTOP SECRET NSA Inspector General Report On Email & Internet Data Collection Under Stellar WindLeakSourceInfoNoch keine Bewertungen
- QoS Issues With Focus On Wireless Body Area NetworksDokument7 SeitenQoS Issues With Focus On Wireless Body Area NetworksTabassumWaheedNoch keine Bewertungen
- Recording Microwave Hearing EffectsDokument8 SeitenRecording Microwave Hearing EffectsJenniferNoch keine Bewertungen
- Kyusun Choi 2010Dokument31 SeitenKyusun Choi 2010mjrsudhakarNoch keine Bewertungen
- (Sawan, Salam, Et All) Wireless Recording Systems From Noninvasive EEG-NIRS To Invasive EEG DevicesDokument10 Seiten(Sawan, Salam, Et All) Wireless Recording Systems From Noninvasive EEG-NIRS To Invasive EEG DevicesJoana Marini De Oliveira CoutoNoch keine Bewertungen
- Brain Implant Victims - MCRAISDokument11 SeitenBrain Implant Victims - MCRAISProjekt_-stop-tortureNoch keine Bewertungen
- Strahlenfolter Stalking - TI - V2K - Movies - Gangstalking - Electronic Harassment - Voice To Skull - Implants - Hearingvoices-Is-VoicetoskullDokument5 SeitenStrahlenfolter Stalking - TI - V2K - Movies - Gangstalking - Electronic Harassment - Voice To Skull - Implants - Hearingvoices-Is-VoicetoskullHans-Georg-JakobsonNoch keine Bewertungen
- The Relative Nature of Low Probability of Detection Radar: A Countermeasures PerspectiveDokument36 SeitenThe Relative Nature of Low Probability of Detection Radar: A Countermeasures PerspectiveamenendezamNoch keine Bewertungen
- IoTSecuritySurvey Final PDFDokument33 SeitenIoTSecuritySurvey Final PDFsantiagogf89Noch keine Bewertungen
- EETimes July-August 2012Dokument56 SeitenEETimes July-August 2012Brzata PticaNoch keine Bewertungen
- Brain-Computer Interface PDFDokument35 SeitenBrain-Computer Interface PDFManoj PradhanNoch keine Bewertungen
- RfidDokument3 SeitenRfidRangaprasad NallapaneniNoch keine Bewertungen
- Combining BCI With Virtual Reality: Towards New Applications and Improved BCIDokument25 SeitenCombining BCI With Virtual Reality: Towards New Applications and Improved BCIMiaStilo AccesoriNoch keine Bewertungen
- G.Hathaway HutchisonEffect PDFDokument25 SeitenG.Hathaway HutchisonEffect PDFjmulder1Noch keine Bewertungen
- Pdfeetesep 2015Dokument70 SeitenPdfeetesep 2015mikadahlNoch keine Bewertungen
- Informatics and Consciousness TransferDokument13 SeitenInformatics and Consciousness TransferSylvia CheungNoch keine Bewertungen
- 16-cv-4014 - CATERBONE v. The United States of America, Et - Al., COMPLAINT July 20, 2016 Ver 3.0 Full With Forms July 22, 2016Dokument448 Seiten16-cv-4014 - CATERBONE v. The United States of America, Et - Al., COMPLAINT July 20, 2016 Ver 3.0 Full With Forms July 22, 2016Stan J. CaterboneNoch keine Bewertungen
- "The FBI and CISPES" Select Committee On Intelligence U.S. Senate (1989)Dokument143 Seiten"The FBI and CISPES" Select Committee On Intelligence U.S. Senate (1989)Defending Rights & DissentNoch keine Bewertungen
- Physician Office LaboratoriesDokument22 SeitenPhysician Office LaboratoriesBrenda Dwi AnandhittaNoch keine Bewertungen
- Short Detail of RNM UserDokument2 SeitenShort Detail of RNM UserKunalNoch keine Bewertungen
- Strahlenfolter Stalking - TI - Bibliotecapleyades - Net - Psychotronic Weapons - Brain Manipulation From A DistanceDokument5 SeitenStrahlenfolter Stalking - TI - Bibliotecapleyades - Net - Psychotronic Weapons - Brain Manipulation From A DistanceHans-Georg-JakobsonNoch keine Bewertungen
- Klystron TubeDokument21 SeitenKlystron TubeRavi Kapatel100% (1)
- Pelicanhpc: A Linux Cluster Distribution For Mpi-Based Parallel ComputingDokument9 SeitenPelicanhpc: A Linux Cluster Distribution For Mpi-Based Parallel ComputingforwalrusNoch keine Bewertungen
- Biotelemetry 3.1 Introduction To BiotelemetryDokument11 SeitenBiotelemetry 3.1 Introduction To Biotelemetrysriram128100% (1)
- Medical Instrumentation: TelemetryDokument10 SeitenMedical Instrumentation: TelemetryRam MNoch keine Bewertungen
- Biomedical Telemetry and TelemedicineDokument44 SeitenBiomedical Telemetry and Telemedicinemeryl132110005Noch keine Bewertungen
- Biotelemetry: Dr. Umme Saima Sunny BDS.,PGT (Oms) Msc. Student of Bme KuetDokument21 SeitenBiotelemetry: Dr. Umme Saima Sunny BDS.,PGT (Oms) Msc. Student of Bme KuetMuhammad Muinul IslamNoch keine Bewertungen
- Theory and Applications of Bio TelemetryDokument20 SeitenTheory and Applications of Bio TelemetryHusseinKhalid100% (1)
- Bio TelemetryDokument10 SeitenBio TelemetryeladNoch keine Bewertungen
- BIOTELEMETRYDokument12 SeitenBIOTELEMETRYTamire santhosh mohanNoch keine Bewertungen
- Enhancement of Mobile Tele-Health System Via GSMDokument5 SeitenEnhancement of Mobile Tele-Health System Via GSMarunnehru_aucseNoch keine Bewertungen
- Computer NotesDokument63 SeitenComputer NotesAadhithya PriyaNoch keine Bewertungen
- Ec2301 Kings College VersionDokument5 SeitenEc2301 Kings College VersionAadhithya PriyaNoch keine Bewertungen
- Ec 2301 - Digital CommunicationDokument10 SeitenEc 2301 - Digital CommunicationAadhithya PriyaNoch keine Bewertungen
- Verilog HDLcs 1202 NotesDokument69 SeitenVerilog HDLcs 1202 NotesAadhithya PriyaNoch keine Bewertungen
- ECE348 Circuit Debugging Tips: Check The Microcontroller Control Register SettingsDokument2 SeitenECE348 Circuit Debugging Tips: Check The Microcontroller Control Register SettingsPri SanNoch keine Bewertungen
- Harman Kardon AVR4000 110 210 310 510 2000 3000 5000Dokument78 SeitenHarman Kardon AVR4000 110 210 310 510 2000 3000 5000Ivan MojsaNoch keine Bewertungen
- Expt 8 Act 3 and 5 & ApplicationsDokument5 SeitenExpt 8 Act 3 and 5 & ApplicationsWNoch keine Bewertungen
- Ti21 TC NotesDokument157 SeitenTi21 TC NotesVikas JainNoch keine Bewertungen
- Application Note CTAN #349: Inverting The Sense of Speed Command SignalsDokument6 SeitenApplication Note CTAN #349: Inverting The Sense of Speed Command SignalsSam eagle goodNoch keine Bewertungen
- Evga X79 Motherboard: User GuideDokument35 SeitenEvga X79 Motherboard: User GuideronuildoNoch keine Bewertungen
- ROX000318781 - AF Functional Description For Roxar 2600 MPFMDokument34 SeitenROX000318781 - AF Functional Description For Roxar 2600 MPFMOmar Al SousliNoch keine Bewertungen
- Anritsu - MS2830A Based PMR SolutionsDokument6 SeitenAnritsu - MS2830A Based PMR SolutionsScribdFgNoch keine Bewertungen
- Ultrafast Soft Recovery Rectifier Diode: Product Benefits Product Features Product ApplicationsDokument4 SeitenUltrafast Soft Recovery Rectifier Diode: Product Benefits Product Features Product ApplicationsEDER RIBEIRONoch keine Bewertungen
- NGR Installation GuideDokument10 SeitenNGR Installation Guidemartins73Noch keine Bewertungen
- Chaotic Multiplication Encryption Method For Security-Enhanced COOFDM-OQAM SystemsDokument4 SeitenChaotic Multiplication Encryption Method For Security-Enhanced COOFDM-OQAM Systemskrishna reddyNoch keine Bewertungen
- Computer Architecture - Lecture Notes, Study Material and Important Questions, AnswersDokument4 SeitenComputer Architecture - Lecture Notes, Study Material and Important Questions, AnswersM.V. TV100% (1)
- Tek Probe TutorialDokument13 SeitenTek Probe Tutorialjvs57Noch keine Bewertungen
- Adoc - Pub SMP Kelas 9 Fisika Bab 2 Rangkaian Listrik Dan SumDokument37 SeitenAdoc - Pub SMP Kelas 9 Fisika Bab 2 Rangkaian Listrik Dan Sumno replayNoch keine Bewertungen
- Simple Agelesss Methods For Field Testing Power TransformersDokument13 SeitenSimple Agelesss Methods For Field Testing Power Transformersraza239Noch keine Bewertungen
- SE-797.2 ARTICLE 23 Standard Practice For Measuring Thickness by Manual Ultrasonic Pulse-Echo Contact MethodDokument8 SeitenSE-797.2 ARTICLE 23 Standard Practice For Measuring Thickness by Manual Ultrasonic Pulse-Echo Contact MethodSean LavergneNoch keine Bewertungen
- Electrical SystemsDokument2 SeitenElectrical SystemsMārcis RancānsNoch keine Bewertungen
- Analog Communication Exam Paper T2 PDFDokument7 SeitenAnalog Communication Exam Paper T2 PDFvavaNoch keine Bewertungen
- Devices and Communication Buses For Devices NetworkDokument211 SeitenDevices and Communication Buses For Devices NetworkDhrumeet PatelNoch keine Bewertungen
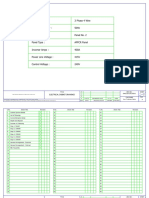
- Apfc Panel DrawingDokument14 SeitenApfc Panel DrawingPRATIKPATELNoch keine Bewertungen
- DDR TI GuidelinesDokument41 SeitenDDR TI Guidelinesnusha aNoch keine Bewertungen
- ENA EREC S36 Extract 180902050402Dokument5 SeitenENA EREC S36 Extract 180902050402MehrdadNoch keine Bewertungen
- Tutorial Sheet FET AmplifierDokument6 SeitenTutorial Sheet FET AmplifierGauravKumarNoch keine Bewertungen
- Pic Microcontroller Based 3 Phase Induction Motor Protection SystemDokument5 SeitenPic Microcontroller Based 3 Phase Induction Motor Protection SystemNaveen ChandarNoch keine Bewertungen
- Millman's Theorem: Chapter 10 - DC Network AnalysisDokument17 SeitenMillman's Theorem: Chapter 10 - DC Network AnalysisAce Dela CruzNoch keine Bewertungen
- Danfoss VLT Aqua Drive Fc202Dokument98 SeitenDanfoss VLT Aqua Drive Fc202api-3696336Noch keine Bewertungen
- Testing PTP Boundary ClocksDokument9 SeitenTesting PTP Boundary ClocksPOC TELKOMSELNoch keine Bewertungen
- LonWorks Design Guide BRDokument14 SeitenLonWorks Design Guide BRasifaliabidNoch keine Bewertungen
- SEW Eurodrive EMS Systems PDFDokument15 SeitenSEW Eurodrive EMS Systems PDFRikardo AlexisNoch keine Bewertungen
- TimemjimpsecondsemDokument2 SeitenTimemjimpsecondsemSundar SharathNoch keine Bewertungen
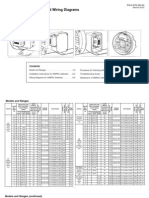
- Installation Instructions and Wiring Diagrams For All Models and RangesDokument8 SeitenInstallation Instructions and Wiring Diagrams For All Models and RangesMaria MusyNoch keine Bewertungen