Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- User Guide RICOH Multi PrinterDokument17 SeitenUser Guide RICOH Multi PrinterKorina AngelaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Kasingkahulugan at KasalungatDokument2 SeitenKasingkahulugan at KasalungatAlfredo Perez73% (11)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Kangen Water TherapiesDokument24 SeitenKangen Water TherapiesKorina Angela100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Anat Physio LarynxDokument7 SeitenAnat Physio LarynxKorina AngelaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Dysphagia PSGDokument53 SeitenDysphagia PSGKartika Sudrajat Budi SetiawanNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Cranial Nerve ExaminationDokument9 SeitenCranial Nerve ExaminationKorina AngelaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Cranial Nerve ExaminationDokument9 SeitenCranial Nerve ExaminationKorina AngelaNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- C1 - Brief History and Background of BadmintonDokument7 SeitenC1 - Brief History and Background of BadmintonKorina AngelaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Pain Myth PDFDokument300 SeitenPain Myth PDFtLzmS23Noch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Fixing My Gaze: A Scientist's Journey Into Seeing in Three DimensionsDokument2 SeitenFixing My Gaze: A Scientist's Journey Into Seeing in Three DimensionsIvan ZamoranoNoch keine Bewertungen
- Measuring Customer Satisfaction at 5 Floor Beauty SalonDokument40 SeitenMeasuring Customer Satisfaction at 5 Floor Beauty SalonIsha MohantyNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- God's For-BEAR-ance With Bullies-Condensed VersionDokument205 SeitenGod's For-BEAR-ance With Bullies-Condensed VersionPatricia BackoraNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Jacobsson Female Gaze PDFDokument26 SeitenJacobsson Female Gaze PDFZina Mechiat100% (2)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Sir Garnel Lesson Plan 1Dokument3 SeitenSir Garnel Lesson Plan 1api-339350946Noch keine Bewertungen
- English, Analogy-Paired Approach Part 4: Suggested TechniqueDokument39 SeitenEnglish, Analogy-Paired Approach Part 4: Suggested TechniquecellyNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Bank Clerk Appraisal FormDokument4 SeitenBank Clerk Appraisal Formpinky_bio878057100% (1)
- The Advaitic Theism of The Bhagavata Purana PDFDokument95 SeitenThe Advaitic Theism of The Bhagavata Purana PDFGerman Burgos100% (1)
- 3 Industrial Training Report FormatDokument6 Seiten3 Industrial Training Report FormatbukhrosliNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Lesson 5 Freedom of The Human PersonDokument8 SeitenLesson 5 Freedom of The Human PersonTotep Reyes75% (4)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- 10 Rockefeller Habits - BriefDokument4 Seiten10 Rockefeller Habits - BriefMeetu SharmaNoch keine Bewertungen
- The Sorrows of Young Werther - Johann Wolfgang Von Goethe PDFDokument78 SeitenThe Sorrows of Young Werther - Johann Wolfgang Von Goethe PDFGary InthNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Media Relations StrategyDokument18 SeitenMedia Relations StrategyBolaji Okusaga100% (1)
- Getting Upstream PDFDokument23 SeitenGetting Upstream PDFMiguel DavillaNoch keine Bewertungen
- Digit SpanDokument10 SeitenDigit SpanshanNoch keine Bewertungen
- Research-G2-12-Gas-C-Chapter 1-3Dokument24 SeitenResearch-G2-12-Gas-C-Chapter 1-3Nicole Ann BaroniaNoch keine Bewertungen
- Research Experience 9781506325125Dokument505 SeitenResearch Experience 9781506325125Cameron AaronNoch keine Bewertungen
- Book Level Ii PDFDokument11 SeitenBook Level Ii PDFMaria Alvarez AmayaNoch keine Bewertungen
- Attention-Deficit Hyperactivity Disorder: A Handbook For Diagnosis and Treatment (4th Ed.)Dokument4 SeitenAttention-Deficit Hyperactivity Disorder: A Handbook For Diagnosis and Treatment (4th Ed.)JANICE JOSEPHINE TJONDROWIBOWO 11-S3Noch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- ASYN Rodriguez PN. EssayDokument1 SeiteASYN Rodriguez PN. EssayNatalie SerranoNoch keine Bewertungen
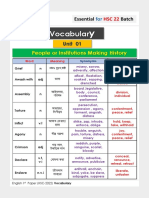
- Vocabulary HSC 22 PDFDokument28 SeitenVocabulary HSC 22 PDFMadara Uchiha83% (6)
- Tara Westrate: 6100 Plainfield Avenue Kalamazoo, Mi 49048Dokument3 SeitenTara Westrate: 6100 Plainfield Avenue Kalamazoo, Mi 49048api-253874188Noch keine Bewertungen
- Lifelong Learning Notes: From LIFELONG LEARNING AND HIGHER EDUCATION Christopher K Knapper, Arthur J CropleyDokument3 SeitenLifelong Learning Notes: From LIFELONG LEARNING AND HIGHER EDUCATION Christopher K Knapper, Arthur J CropleyGe VergaNoch keine Bewertungen
- Test 1 - Identification (2 Points Each) : Bugo National High School-SHSDokument2 SeitenTest 1 - Identification (2 Points Each) : Bugo National High School-SHSNamja Ileum Ozara GaabucayanNoch keine Bewertungen
- Oliver Twist Chapter 9-12 - UpdatedDokument21 SeitenOliver Twist Chapter 9-12 - UpdatedBee FeeNoch keine Bewertungen
- A Study On Vocational Needs of Inmates of Government Childrens Homes in KeralaDokument11 SeitenA Study On Vocational Needs of Inmates of Government Childrens Homes in KeralaIJAR JOURNALNoch keine Bewertungen
- Session Guide For Knowledge ChannelDokument3 SeitenSession Guide For Knowledge ChannelIvan GunoNoch keine Bewertungen
- Themes QuotesDokument4 SeitenThemes QuotesAishi GuptaNoch keine Bewertungen
- Academic Writing - Introduction (COLL)Dokument21 SeitenAcademic Writing - Introduction (COLL)Kainat BatoolNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)