Das könnte Ihnen auch gefallen
- Sleep Disorders in Selected Psychiatric Settings: A Clinical CasebookVon EverandSleep Disorders in Selected Psychiatric Settings: A Clinical CasebookImran S. KhawajaNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 12: NeurologyVon EverandComplementary and Alternative Medical Lab Testing Part 12: NeurologyNoch keine Bewertungen
- Comorbid Anxiety and Depression - Epidemiology, Clinical Manifestations, and Diagnosis PDFDokument24 SeitenComorbid Anxiety and Depression - Epidemiology, Clinical Manifestations, and Diagnosis PDFdreaming0% (1)
- Barrett Impulsiveness Scale (BIS-11)Dokument10 SeitenBarrett Impulsiveness Scale (BIS-11)andr3yl0Noch keine Bewertungen
- Apego Transgeneracional y AnorexiaDokument9 SeitenApego Transgeneracional y AnorexiaadriNoch keine Bewertungen
- 1 s2.0 S152550502300135X MainDokument8 Seiten1 s2.0 S152550502300135X MainilonaskorinNoch keine Bewertungen
- A Survey of Sleep Habits and Sleeping Difficulties in An Elderly Swedish PopulationDokument14 SeitenA Survey of Sleep Habits and Sleeping Difficulties in An Elderly Swedish PopulationPriyanshuNoch keine Bewertungen
- Epidemiology of Insomnia: Prevalence and Risk FactorsDokument22 SeitenEpidemiology of Insomnia: Prevalence and Risk Factorsshf.mxlikNoch keine Bewertungen
- Prevalence of Psychiatric Disorders in Infertile Women and Men Undergoing in Vitro Fertilization TreatmentDokument8 SeitenPrevalence of Psychiatric Disorders in Infertile Women and Men Undergoing in Vitro Fertilization TreatmentMaria Galia Elias QuirogaNoch keine Bewertungen
- Ansiedad y DepresionDokument21 SeitenAnsiedad y DepresionEdgar AvilésNoch keine Bewertungen
- 2011 - IJCHP - The Leyton Obsessional Inventory-Child VersionDokument16 Seiten2011 - IJCHP - The Leyton Obsessional Inventory-Child VersionEsteysi Villarroel BernalesNoch keine Bewertungen
- Demencia en Gente Muy MayorDokument6 SeitenDemencia en Gente Muy MayorJimenaNoch keine Bewertungen
- Anxiety Disorders Among Adolescents Referred To General Psychiatry For Multiple Causes: Clinical Presentation, Prevalence, and ComorbidityDokument10 SeitenAnxiety Disorders Among Adolescents Referred To General Psychiatry For Multiple Causes: Clinical Presentation, Prevalence, and ComorbidityRatu CalistaNoch keine Bewertungen
- Research Articles: Childhood Adversity and Vulnerability To Mood and Anxiety DisordersDokument7 SeitenResearch Articles: Childhood Adversity and Vulnerability To Mood and Anxiety DisordersMifta 'hera' Khaerati IINoch keine Bewertungen
- Cannabis Paper 2Dokument6 SeitenCannabis Paper 2Carlos Eduardo Jorquera GonzálezNoch keine Bewertungen
- C SCL-90: Onfiabilidad Y Validez DE LA EN LA Evaluación DE Psicopatología EN MujeresDokument9 SeitenC SCL-90: Onfiabilidad Y Validez DE LA EN LA Evaluación DE Psicopatología EN MujeresGarcía JuanNoch keine Bewertungen
- Cancer Information Overload and Death Anxiety Predict Health AnxietyDokument8 SeitenCancer Information Overload and Death Anxiety Predict Health AnxietyRobynNoch keine Bewertungen
- Lehtinen 1994Dokument4 SeitenLehtinen 1994HARINI KNoch keine Bewertungen
- Anxiety Disorder Symptoms in Children and Adolescents: Differences by Age and Gender in A Community SampleDokument6 SeitenAnxiety Disorder Symptoms in Children and Adolescents: Differences by Age and Gender in A Community SampleJesús Rafael Méndez NateraNoch keine Bewertungen
- Barlow Et Al 1984Dokument19 SeitenBarlow Et Al 1984290971Noch keine Bewertungen
- Swinkels PscychopathologieDokument16 SeitenSwinkels PscychopathologiesezalwickNoch keine Bewertungen
- Rosario V-1 - Agosto20Dokument8 SeitenRosario V-1 - Agosto20Lupita LópezNoch keine Bewertungen
- Behavioral and Emotional Effects of Repeated General Anesthesia in Young ChildrenDokument1 SeiteBehavioral and Emotional Effects of Repeated General Anesthesia in Young ChildrenRogger MagallanesNoch keine Bewertungen
- Depression, Alzheimer, Family CaregiversDokument13 SeitenDepression, Alzheimer, Family CaregiversCathy Georgiana HNoch keine Bewertungen
- An Investigation of Irrational Beliefs and Death Anxiety As A Function of Hiv StatusDokument18 SeitenAn Investigation of Irrational Beliefs and Death Anxiety As A Function of Hiv StatusDana PascuNoch keine Bewertungen
- Affective DisordersDokument37 SeitenAffective Disordersveronicaine91Noch keine Bewertungen
- Anxiety Symptoms in Adolescents at RiskDokument5 SeitenAnxiety Symptoms in Adolescents at RiskifclarinNoch keine Bewertungen
- Anxiety and Depression Are Risk Factors Rather Than Consequences of Functional Somatic Symptoms in A General Population of Adolescents - The TRAILS StudyDokument9 SeitenAnxiety and Depression Are Risk Factors Rather Than Consequences of Functional Somatic Symptoms in A General Population of Adolescents - The TRAILS StudyJPCP 2014Noch keine Bewertungen
- Depressive Disorders in Epilepsy: SummaryDokument4 SeitenDepressive Disorders in Epilepsy: SummaryRadi PdNoch keine Bewertungen
- Suicidal Intension Among Depresssion pts.-1Dokument18 SeitenSuicidal Intension Among Depresssion pts.-1Firdouse ShajiNoch keine Bewertungen
- Identification and Pychological Treament of Adolescent Panic Disorder 2020Dokument8 SeitenIdentification and Pychological Treament of Adolescent Panic Disorder 2020Almudena RodriguezNoch keine Bewertungen
- Álvarez Et Al (2011) ChildabuseDokument6 SeitenÁlvarez Et Al (2011) ChildabuseAra Moreno EscaladaNoch keine Bewertungen
- Anxiety and Mood Disorders in Narcolepsy: A Case - Control StudyDokument8 SeitenAnxiety and Mood Disorders in Narcolepsy: A Case - Control StudyDesyifa Annisa MursalinNoch keine Bewertungen
- Prev Ans Depr CanverDokument6 SeitenPrev Ans Depr CanverÉrico AugustoNoch keine Bewertungen
- Kurre 2012 - Gender Perceived Disability Anxiety Depression 1472-6815-12-2Dokument12 SeitenKurre 2012 - Gender Perceived Disability Anxiety Depression 1472-6815-12-2Ikhsan JohnsonNoch keine Bewertungen
- Duration of Depressive Symptoms and Mortality Risk The English Longitudinal Study of Ageing ElsaDokument6 SeitenDuration of Depressive Symptoms and Mortality Risk The English Longitudinal Study of Ageing ElsaAishwarya PuttaNoch keine Bewertungen
- Art 3A10.1007 2Fs10862 011 9224 yDokument8 SeitenArt 3A10.1007 2Fs10862 011 9224 yastrimentariNoch keine Bewertungen
- 4 Gotlib2014Dokument18 Seiten4 Gotlib2014Javiera Luna Marcel Zapata-SalazarNoch keine Bewertungen
- Ansiedad Comorbilidad en Epi KannerDokument2 SeitenAnsiedad Comorbilidad en Epi Kannerkarina fontanezNoch keine Bewertungen
- Marital Status and Risk For Late LifeDokument13 SeitenMarital Status and Risk For Late LifeHargo PsyNoch keine Bewertungen
- Depression in Children AdolescentsDokument7 SeitenDepression in Children AdolescentstoddhavelkaNoch keine Bewertungen
- Suicide Epilepsy CohortDokument10 SeitenSuicide Epilepsy CohortDiana SelaruNoch keine Bewertungen
- JournalDokument6 SeitenJournalWisnu AdhanantyoNoch keine Bewertungen
- Original Paper Comorbidity of Epilepsy and Depression in Al Husseini Teaching Hospital in Holy Kerbala /iraq in 2018Dokument9 SeitenOriginal Paper Comorbidity of Epilepsy and Depression in Al Husseini Teaching Hospital in Holy Kerbala /iraq in 2018sarhang talebaniNoch keine Bewertungen
- Psychiatric Comorbidities Among Adolescents With and Without Anxiety Disorders: A Community StudyDokument6 SeitenPsychiatric Comorbidities Among Adolescents With and Without Anxiety Disorders: A Community StudyLiliana PonteNoch keine Bewertungen
- Yahia2013 Article PredictorsOfAnxietyAndDepressiDokument6 SeitenYahia2013 Article PredictorsOfAnxietyAndDepressiamasoud96 amasoud96Noch keine Bewertungen
- Prevalence and Predictors of Depression Amongst ElderlyDokument4 SeitenPrevalence and Predictors of Depression Amongst ElderlyDr.Wajid Habib (Doxxsab)Noch keine Bewertungen
- Antipsychotic Medication Induced Movement Disorders: The Case of Amanuel Specialized Mental Hospital, Addis Ababa, EthiopiaDokument7 SeitenAntipsychotic Medication Induced Movement Disorders: The Case of Amanuel Specialized Mental Hospital, Addis Ababa, Ethiopiael egendNoch keine Bewertungen
- Schizophr Bull 1994 Gordon 697 712Dokument16 SeitenSchizophr Bull 1994 Gordon 697 712EdwardVargasNoch keine Bewertungen
- Alfano, Ginsburg, & Kingery (2007) SleepDokument9 SeitenAlfano, Ginsburg, & Kingery (2007) SleepJanuaryska SaraswatiNoch keine Bewertungen
- Do Different Orthodontic Malocclusions Affect Patients' Self-Concept and Psychosocial Status?Dokument4 SeitenDo Different Orthodontic Malocclusions Affect Patients' Self-Concept and Psychosocial Status?Claypella MaskNoch keine Bewertungen
- Correlatos Del Maltrato Físico en La Infancia en Mujeres Adultas Con Trastorno Distímico o Depresión MayorDokument8 SeitenCorrelatos Del Maltrato Físico en La Infancia en Mujeres Adultas Con Trastorno Distímico o Depresión MayormagdaNoch keine Bewertungen
- Content ServerDokument11 SeitenContent ServerTriismyNoch keine Bewertungen
- Definition of InsomniaDokument10 SeitenDefinition of Insomniaeka yusrianaNoch keine Bewertungen
- 87-5 Retardasi MentalDokument7 Seiten87-5 Retardasi MentalShalawatyAbdkarimNoch keine Bewertungen
- Psychopharmacology of AutismDokument17 SeitenPsychopharmacology of AutismMichelle2Noch keine Bewertungen
- Chang 2018Dokument14 SeitenChang 2018spaciugNoch keine Bewertungen
- Visual Height Intolerance and Acrophobia: Distressing Partners For LifeDokument8 SeitenVisual Height Intolerance and Acrophobia: Distressing Partners For LifeAnonymous OCVES8U7Noch keine Bewertungen
- Social Science & Medicine: ReviewDokument17 SeitenSocial Science & Medicine: ReviewNabellaNoch keine Bewertungen
- The Developmental Epidemiology of Anxiety Disorders Phenomenology, Prevalence, and ComorbityDokument18 SeitenThe Developmental Epidemiology of Anxiety Disorders Phenomenology, Prevalence, and ComorbityShirleuy GonçalvesNoch keine Bewertungen
- Resveratrol and Glucose ControlDokument10 SeitenResveratrol and Glucose ControlDian Isti AngrainiNoch keine Bewertungen
- Breastfeeding en Women WorkDokument7 SeitenBreastfeeding en Women WorkDian Isti AngrainiNoch keine Bewertungen
- Resveratrol and CA ColonDokument6 SeitenResveratrol and CA ColonDian Isti AngrainiNoch keine Bewertungen
- Jurnal-3-Naskah 5 JURNAL PDGI Vol 59 No 1Dokument5 SeitenJurnal-3-Naskah 5 JURNAL PDGI Vol 59 No 1Bruno Adiputra Patut IINoch keine Bewertungen
- Epilepsi JaksonDokument1 SeiteEpilepsi JaksonDian Isti AngrainiNoch keine Bewertungen
- All About InjectionDokument24 SeitenAll About InjectionDian Isti AngrainiNoch keine Bewertungen
- Poststroke EpilepsyDokument5 SeitenPoststroke EpilepsyDian Isti AngrainiNoch keine Bewertungen
- Poststroke EpilepsyDokument5 SeitenPoststroke EpilepsyDian Isti AngrainiNoch keine Bewertungen
- Seizstroke in ChildDokument6 SeitenSeizstroke in ChildDian Isti AngrainiNoch keine Bewertungen
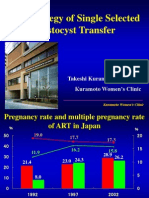
- The Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDokument43 SeitenThe Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDian Isti AngrainiNoch keine Bewertungen
- Malnutrition Elderly Quick Ref GuideDokument4 SeitenMalnutrition Elderly Quick Ref GuideDian Isti AngrainiNoch keine Bewertungen
- Jurnal PDFDokument10 SeitenJurnal PDFNayda FitrinaNoch keine Bewertungen
- 11821116Dokument10 Seiten11821116Dian Isti AngrainiNoch keine Bewertungen
- 1949 Winnicott Hate in The CountertransferenceDokument10 Seiten1949 Winnicott Hate in The CountertransferenceKevin McInnes100% (1)
- Name M Jalil Khan Reg No Bscn02161014 NCP (Insomnia) Assessment Diagnosis Planning Intervention Rational Evaluation Short TermDokument2 SeitenName M Jalil Khan Reg No Bscn02161014 NCP (Insomnia) Assessment Diagnosis Planning Intervention Rational Evaluation Short TermNargis MughalNoch keine Bewertungen
- Product Details: Medicine Mcqs For Medical Professionals PDFDokument2 SeitenProduct Details: Medicine Mcqs For Medical Professionals PDFUtkarsh SharmaNoch keine Bewertungen
- Spitzer, R. L. Et Al (2006) A Brief Measure For Assessing Generalized Anxiety Disorder - The GAD-7Dokument6 SeitenSpitzer, R. L. Et Al (2006) A Brief Measure For Assessing Generalized Anxiety Disorder - The GAD-7Kristopher MacKenzie BrignardelloNoch keine Bewertungen
- Assignment 40Dokument27 SeitenAssignment 40vasisth50Noch keine Bewertungen
- Annotated BibDokument6 SeitenAnnotated Bibapi-194035532Noch keine Bewertungen
- STOP, LOOK, AND LISTEN: The Challenge For Children With ADHDDokument13 SeitenSTOP, LOOK, AND LISTEN: The Challenge For Children With ADHDJFNoch keine Bewertungen
- Artigos Aaron BeckDokument32 SeitenArtigos Aaron BeckstragusrjNoch keine Bewertungen
- Donna Williams Interview PDFDokument8 SeitenDonna Williams Interview PDFDiego Yonathan Moreno RamirezNoch keine Bewertungen
- Substance Abuse Group ProjectDokument9 SeitenSubstance Abuse Group Projectapi-253915117Noch keine Bewertungen
- Pitman 2002 Biological-PsychiatryDokument4 SeitenPitman 2002 Biological-PsychiatryQwerty QwertyNoch keine Bewertungen
- NICHQ Vanderbilt Teacher RatingDokument3 SeitenNICHQ Vanderbilt Teacher RatingJanine Erica De LunaNoch keine Bewertungen
- A Mental Healthcare Model For Mass Trauma Survivors - M. Basoglu, Et. Al., (Cambridge, 2011) WW PDFDokument296 SeitenA Mental Healthcare Model For Mass Trauma Survivors - M. Basoglu, Et. Al., (Cambridge, 2011) WW PDFraulNoch keine Bewertungen
- PAAM LecturesDokument167 SeitenPAAM LecturesekyecNoch keine Bewertungen
- Attachment Trauma and Multiplicity Working With Dissociative Identity DisorderDokument241 SeitenAttachment Trauma and Multiplicity Working With Dissociative Identity DisorderDaedalusNoch keine Bewertungen
- Wender Utah Rating Scale (Wurs) : As A Child I Was (Or Had)Dokument2 SeitenWender Utah Rating Scale (Wurs) : As A Child I Was (Or Had)J31415Noch keine Bewertungen
- Girl InterruptedDokument7 SeitenGirl Interruptedapi-365678992Noch keine Bewertungen
- Mental Health Nurse CVDokument2 SeitenMental Health Nurse CVTimur UrakovNoch keine Bewertungen
- Name of The Hospital - Teaching Hospital, Karapitiya: Case 7 Puerperal PsychosisDokument13 SeitenName of The Hospital - Teaching Hospital, Karapitiya: Case 7 Puerperal PsychosisCharith Rukmal KodituwakkuNoch keine Bewertungen
- Clinical Ethics For The Treatment of Children and AdolescentsDokument15 SeitenClinical Ethics For The Treatment of Children and AdolescentsPierre AA100% (1)
- 7718 (07) Review of Cases - Anxiety DisordersDokument34 Seiten7718 (07) Review of Cases - Anxiety DisordersnewazNoch keine Bewertungen
- Theoretical Perspectives in CounselingDokument28 SeitenTheoretical Perspectives in CounselingGargi BishtNoch keine Bewertungen
- Ed WilliamsDokument39 SeitenEd WilliamsTamara BatesNoch keine Bewertungen
- CBT Labelling EmotionsDokument3 SeitenCBT Labelling Emotionskicaanu100% (1)
- Attachment Theory: Summary: Attachment Theory Emphasizes The Importance of A Secure and Trusting Mother-Infant BondDokument3 SeitenAttachment Theory: Summary: Attachment Theory Emphasizes The Importance of A Secure and Trusting Mother-Infant BondRessie Joy Catherine Felices100% (2)
- Mcmi Iii Report JamilDokument8 SeitenMcmi Iii Report Jamilshubhangi kapoor100% (1)
- 12steps To Creating Motivation When DepressedDokument3 Seiten12steps To Creating Motivation When DepressedAnonymous Ax12P2srNoch keine Bewertungen
- Phobia EssayDokument4 SeitenPhobia EssayEdna MartinezNoch keine Bewertungen
- Sensory Abnormalities in Children With Autism SpecDokument9 SeitenSensory Abnormalities in Children With Autism SpecceavilaNoch keine Bewertungen