Das könnte Ihnen auch gefallen
- Harvard School of Public Health Health and Society Ph201X Instructors Faculty Lead: Ichiro Kawachi, MD, PHDDokument8 SeitenHarvard School of Public Health Health and Society Ph201X Instructors Faculty Lead: Ichiro Kawachi, MD, PHDmarkkkkkkkheeessNoch keine Bewertungen
- 1 PDFDokument77 Seiten1 PDFmarkkkkkkkheeessNoch keine Bewertungen
- 16 WHO Health Systems Financing WDR 2010Dokument12 Seiten16 WHO Health Systems Financing WDR 2010markkkkkkkheeessNoch keine Bewertungen
- Sample Academic MEMODokument1 SeiteSample Academic MEMOmarkkkkkkkheeessNoch keine Bewertungen
- Ra 10354 PDFDokument24 SeitenRa 10354 PDFmarkkkkkkkheeessNoch keine Bewertungen
- Abstract Submission Form 2018 PPA ConferenceDokument2 SeitenAbstract Submission Form 2018 PPA ConferencemarkkkkkkkheeessNoch keine Bewertungen
- 05 Yasuhiko Saito Japanese Longitudinal Study of AgingDokument79 Seiten05 Yasuhiko Saito Japanese Longitudinal Study of AgingmarkkkkkkkheeessNoch keine Bewertungen
- Introduction and Overview: Data Scientist: The Sexiest Job of The 21st CenturyDokument13 SeitenIntroduction and Overview: Data Scientist: The Sexiest Job of The 21st CenturymarkkkkkkkheeessNoch keine Bewertungen
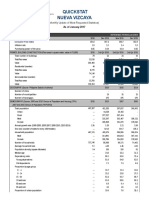
- Quickstat Nueva Vizcaya: (Monthly Update of Most Requested Statistics)Dokument5 SeitenQuickstat Nueva Vizcaya: (Monthly Update of Most Requested Statistics)markkkkkkkheeessNoch keine Bewertungen
- Lecture16 PDFDokument27 SeitenLecture16 PDFmarkkkkkkkheeessNoch keine Bewertungen
- 101 Health Research Template Ethical ConsiderationsDokument2 Seiten101 Health Research Template Ethical ConsiderationsmarkkkkkkkheeessNoch keine Bewertungen
- Continuous Data MeasuresDokument16 SeitenContinuous Data MeasuresmarkkkkkkkheeessNoch keine Bewertungen
- Independent Variables Living ArrangementDokument1 SeiteIndependent Variables Living ArrangementmarkkkkkkkheeessNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- BSSC 112 Introduction To Psychology PDFDokument150 SeitenBSSC 112 Introduction To Psychology PDFMushaa DherreNoch keine Bewertungen
- Differentiation and Enrichment Strategies For Gifted StudentsDokument4 SeitenDifferentiation and Enrichment Strategies For Gifted Studentsapi-448710928Noch keine Bewertungen
- St. Joseph'S College of Commerce: Post Graduate DepartmentDokument22 SeitenSt. Joseph'S College of Commerce: Post Graduate DepartmentShruti AshokNoch keine Bewertungen
- Counseling TestDokument11 SeitenCounseling Testnovie100% (1)
- Action Plan SSG PDFDokument2 SeitenAction Plan SSG PDFLove Shore0% (2)
- The Writings of Milton H. Erickson by Harry Procter (2001) : January 2001Dokument17 SeitenThe Writings of Milton H. Erickson by Harry Procter (2001) : January 2001Giorgi TakidzeNoch keine Bewertungen
- Mendelsohn Analytic LoveDokument27 SeitenMendelsohn Analytic Lovealb_books100% (2)
- Guidelines For Inpatient Pharmacy PracticeDokument68 SeitenGuidelines For Inpatient Pharmacy PracticeAmir Ihsan100% (1)
- Introduction To Transactional AnalysisDokument26 SeitenIntroduction To Transactional AnalysisPeter Creagh100% (18)
- Autistic Schizophrenic Children: An Experiment in The Use of LSD-25Dokument11 SeitenAutistic Schizophrenic Children: An Experiment in The Use of LSD-25VDNoch keine Bewertungen
- Shedler (2006) That Was Then, This Is Now PDFDokument59 SeitenShedler (2006) That Was Then, This Is Now PDFGil GonzálezNoch keine Bewertungen
- Sociocultural PerspectiveDokument11 SeitenSociocultural PerspectiveadeshNoch keine Bewertungen
- Advenst and PsychiatryDokument67 SeitenAdvenst and PsychiatryAdalene SalesNoch keine Bewertungen
- Social Work CourseworkDokument7 SeitenSocial Work Courseworkf675ztsf100% (2)
- Watling Dietz 2007 SI Immediate Effect of Intervention Autism Ss Design PDFDokument10 SeitenWatling Dietz 2007 SI Immediate Effect of Intervention Autism Ss Design PDFKiyorNoch keine Bewertungen
- Aleosan National High SchoolDokument4 SeitenAleosan National High SchoolFaith InsoyNoch keine Bewertungen
- Itl600 Week 3 Collaborative Group AssignmentDokument11 SeitenItl600 Week 3 Collaborative Group Assignmentapi-423232776Noch keine Bewertungen
- Social ActionDokument5 SeitenSocial ActionsydnaxNoch keine Bewertungen
- DBT Cope Ahead PlanDokument1 SeiteDBT Cope Ahead PlanAmy PowersNoch keine Bewertungen
- Model of Human OccupationDokument6 SeitenModel of Human OccupationOvidiu MunteanNoch keine Bewertungen
- ILM Level 5 CC& MM - Enrolment Letter - April 2009 ProgrammeDokument5 SeitenILM Level 5 CC& MM - Enrolment Letter - April 2009 ProgrammeproxyelevNoch keine Bewertungen
- The Mind Guide To Seeking Help For A Mental Health ProblemDokument32 SeitenThe Mind Guide To Seeking Help For A Mental Health ProblemRobbieD455Noch keine Bewertungen
- Pine - Four PsychologiesDokument21 SeitenPine - Four Psychologieslaura100% (1)
- The Evolution of Circular Questions: Training Family TherapistsDokument15 SeitenThe Evolution of Circular Questions: Training Family TherapistsravhcolNoch keine Bewertungen
- Internet Addiction Scale A Parametric Study EFA MexicoDokument20 SeitenInternet Addiction Scale A Parametric Study EFA MexicoSarai CastrellónNoch keine Bewertungen
- NLP in MotionDokument3 SeitenNLP in MotionSpeech & Language Therapy in PracticeNoch keine Bewertungen
- Pagsulhugon National High School Babatngon, Leyte: Republic of The PhilippinesDokument3 SeitenPagsulhugon National High School Babatngon, Leyte: Republic of The PhilippinesMARIA THERESA M. HERBOLINGONoch keine Bewertungen
- Comer School Development ProgramDokument5 SeitenComer School Development ProgramCTREQ école-famille-communautéNoch keine Bewertungen
- Teen DepressionDokument6 SeitenTeen DepressionDonna Claire AngusNoch keine Bewertungen
- Case ConceptualizationDokument8 SeitenCase ConceptualizationRuby JadeNoch keine Bewertungen