Das könnte Ihnen auch gefallen
- EMQs For Medical Students Volume 3 2eDokument16 SeitenEMQs For Medical Students Volume 3 2ePasTestBooks50% (2)
- EMQs For Medical Students Volume 2 2eDokument30 SeitenEMQs For Medical Students Volume 2 2ePasTestBooks50% (2)
- EMQs For Medical Students Volume 1 2EDokument27 SeitenEMQs For Medical Students Volume 1 2EPasTestBooks100% (2)
- Oscesbook 1Dokument38 SeitenOscesbook 1PasTestBooks100% (1)
- MRCPCH Part 1 Questions With Individual Subject Summaries 4eDokument52 SeitenMRCPCH Part 1 Questions With Individual Subject Summaries 4ePasTestBooks88% (25)
- Data Interpretation For Medical StudentsDokument42 SeitenData Interpretation For Medical StudentsPasTestBooks100% (6)
- MRCPCH Clinical: Short Cases, History Taking & Communication Skills 3eDokument19 SeitenMRCPCH Clinical: Short Cases, History Taking & Communication Skills 3ePasTestBooks100% (6)
- MRCP ErnDokument41 SeitenMRCP ErnPasTestBooksNoch keine Bewertungen
- Ern MRCPCHDokument24 SeitenErn MRCPCHPasTestBooksNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Job DescriptionsDokument139 SeitenJob DescriptionsAbdullah Bin SaeedNoch keine Bewertungen
- Aneurysm: Symptoms of An AneurysmDokument3 SeitenAneurysm: Symptoms of An AneurysmArun MuralidharanNoch keine Bewertungen
- Physical Abuse Teaching SlidesDokument19 SeitenPhysical Abuse Teaching SlidesbentoeNoch keine Bewertungen
- A Case Study On MastitisDokument15 SeitenA Case Study On MastitisAnil Sigdel100% (3)
- Suicide in Adolescent - A Case ReportDokument5 SeitenSuicide in Adolescent - A Case ReportRebecca SilaenNoch keine Bewertungen
- Parasitology: - IntroductionDokument62 SeitenParasitology: - IntroductionHana AliNoch keine Bewertungen
- APA Practice Guideline For The Treatment of Patients With Substance Use DisordersDokument276 SeitenAPA Practice Guideline For The Treatment of Patients With Substance Use DisordersRaja Ahmad Rusdan MusyawirNoch keine Bewertungen
- Multiple Personality Disorder: Is It Fact or Fiction?: Deguzman 1Dokument10 SeitenMultiple Personality Disorder: Is It Fact or Fiction?: Deguzman 1Eliza Philline De GuzmanNoch keine Bewertungen
- Travatan (Travoprost Ophthalmic Solution) 0.004% SterileDokument7 SeitenTravatan (Travoprost Ophthalmic Solution) 0.004% SterileSyed Shariq AliNoch keine Bewertungen
- Treating Canine Distemper VirusDokument23 SeitenTreating Canine Distemper VirusJack HollandNoch keine Bewertungen
- Complications of Insulin TherapyDokument16 SeitenComplications of Insulin TherapyIngrid NicolasNoch keine Bewertungen
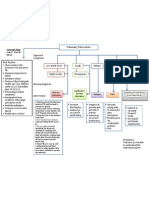
- Concept Map PTBDokument1 SeiteConcept Map PTBJoan Abardo100% (2)
- DctsDokument30 SeitenDctsInuyashayahoo100% (1)
- Radiotherapy in Prostate Cancer Innovative Techniques and Current ControversiesDokument288 SeitenRadiotherapy in Prostate Cancer Innovative Techniques and Current ControversiesStirNoch keine Bewertungen
- PMLSDokument9 SeitenPMLSChan ChanNoch keine Bewertungen
- Dr. Ugi Sugiri, SpEm - PPT OBMED PDFDokument56 SeitenDr. Ugi Sugiri, SpEm - PPT OBMED PDFDaniel Aprianto SihotangNoch keine Bewertungen
- Et TR MedDokument99 SeitenEt TR MedThe ScienceNoch keine Bewertungen
- Bacteria Found in UrineDokument7 SeitenBacteria Found in UrineAria DomingoNoch keine Bewertungen
- Anesthesia-Assessing Depth PDFDokument1 SeiteAnesthesia-Assessing Depth PDFAvinash Technical ServiceNoch keine Bewertungen
- SeizureDokument10 SeitenSeizureRomeo ReyesNoch keine Bewertungen
- Grief TherapyDokument15 SeitenGrief Therapygauri pillaiNoch keine Bewertungen
- Nur 601 - Literature Review Manuscript-Icd-10-Sunny Carrington-HahnDokument22 SeitenNur 601 - Literature Review Manuscript-Icd-10-Sunny Carrington-Hahnapi-357138638Noch keine Bewertungen
- 2020 Anaphylaxis JACI 2020Dokument42 Seiten2020 Anaphylaxis JACI 2020Peter Albeiro Falla CortesNoch keine Bewertungen
- Unit 0000 Topik 9. Word Formation: Nouns: Bold) To Nouns. Do Not Change TheDokument5 SeitenUnit 0000 Topik 9. Word Formation: Nouns: Bold) To Nouns. Do Not Change TheioakasNoch keine Bewertungen
- Editorial: Dental Caries and OsteoporosisDokument2 SeitenEditorial: Dental Caries and OsteoporosisBagis Emre GulNoch keine Bewertungen
- Secukinumab: First Global ApprovalDokument10 SeitenSecukinumab: First Global ApprovalAri KurniawanNoch keine Bewertungen
- Raynaud's DiseaseDokument8 SeitenRaynaud's DiseaseAhmad Barrun NidhomNoch keine Bewertungen
- Case ReportDokument11 SeitenCase ReportBerhanu DigamoNoch keine Bewertungen
- Using Pediatric Pain Scales Neonatal Infant Pain Scale (NIPSDokument2 SeitenUsing Pediatric Pain Scales Neonatal Infant Pain Scale (NIPSSevina Eka ChannelNoch keine Bewertungen