Das könnte Ihnen auch gefallen
- Template For Clinical Progress Note June 2009Dokument3 SeitenTemplate For Clinical Progress Note June 2009Buthaina AltenaijiNoch keine Bewertungen
- Psycholinguistics: Language Disorder: Broca's AphasiaDokument18 SeitenPsycholinguistics: Language Disorder: Broca's AphasiaSuciati AnandesNoch keine Bewertungen
- NCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDokument5 SeitenNCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDud AccNoch keine Bewertungen
- BMC Ultrasound ReportDokument3 SeitenBMC Ultrasound ReportBrandy PorciunculaNoch keine Bewertungen
- Geriatrics AssesmentbysedgeDokument4 SeitenGeriatrics Assesmentbysedgephysio115Noch keine Bewertungen
- UsrsaplettersPre-Employment Medical FormDokument2 SeitenUsrsaplettersPre-Employment Medical FormMahesh Yadav100% (1)
- Patient Encounter FormDokument2 SeitenPatient Encounter FormSpectator Medic0% (1)
- Pre-Employment Medical FormDokument2 SeitenPre-Employment Medical FormSourin NandiNoch keine Bewertungen
- New Assessment ToolDokument9 SeitenNew Assessment Toolneri_pearlNoch keine Bewertungen
- PT Assessment ToolDokument2 SeitenPT Assessment ToolSally GigelioNoch keine Bewertungen
- Obstetric Assessment ToolDokument5 SeitenObstetric Assessment ToolDudil GoatNoch keine Bewertungen
- Botox New Patient PaperworkDokument9 SeitenBotox New Patient PaperworkMAI100% (1)
- New Assessment Form 2Dokument5 SeitenNew Assessment Form 2api-3739910100% (2)
- Newborn Physical AssessmentDokument7 SeitenNewborn Physical AssessmentBinal JoshiNoch keine Bewertungen
- Justisse MethodDokument64 SeitenJustisse Methodtiiandi100% (3)
- HandOff SampleToolsDokument9 SeitenHandOff SampleToolsOllie EvansNoch keine Bewertungen
- Cerebrospinal Fluid: Physical Characteristic and Composition of The Cerebrospinal FluidDokument5 SeitenCerebrospinal Fluid: Physical Characteristic and Composition of The Cerebrospinal FluiderickNoch keine Bewertungen
- Physician Order SheetDokument4 SeitenPhysician Order SheetResci Angelli Rizada-NolascoNoch keine Bewertungen
- Blood Bank QuizDokument13 SeitenBlood Bank Quizdimalawang.af100% (1)
- Pass Ultrasound Physics Exam Review Match the AnswersVon EverandPass Ultrasound Physics Exam Review Match the AnswersBewertung: 4 von 5 Sternen4/5 (4)
- SBAR Labor Delivery Report Hand Off Sheet and Assessment Tool 110411 Update PDFDokument2 SeitenSBAR Labor Delivery Report Hand Off Sheet and Assessment Tool 110411 Update PDFKathleenNoch keine Bewertungen
- Self Declaration - Consent Form Poddar Nursing Home and Hospital Before SuregryDokument12 SeitenSelf Declaration - Consent Form Poddar Nursing Home and Hospital Before SuregryRahul PoddarNoch keine Bewertungen
- Essensial Hypertension Pathogenesis and PathophsiologyDokument22 SeitenEssensial Hypertension Pathogenesis and PathophsiologyAmeliana KamaludinNoch keine Bewertungen
- Asthma Action PlanDokument1 SeiteAsthma Action PlanLeizlNoch keine Bewertungen
- Haad Exam 2017Dokument6 SeitenHaad Exam 2017midhun100% (1)
- Medical PerformaDokument5 SeitenMedical Performamashal naeemNoch keine Bewertungen
- Knee Eval FormDokument3 SeitenKnee Eval Formsoudy ptNoch keine Bewertungen
- Prealb: - Amy/lip: - Lact: - Trop: - UADokument1 SeitePrealb: - Amy/lip: - Lact: - Trop: - UAblackblossom2Noch keine Bewertungen
- Physical Therapy Evaluation FormDokument6 SeitenPhysical Therapy Evaluation FormRobin MathewNoch keine Bewertungen
- Nursing Administration AssessmentDokument6 SeitenNursing Administration Assessmentkatnebrija89Noch keine Bewertungen
- NIMAS Medical FormDokument2 SeitenNIMAS Medical FormBhargav VekariaNoch keine Bewertungen
- Asthma Reactive Airway Exercise Induced Bronchospasm QuestionnaireDokument1 SeiteAsthma Reactive Airway Exercise Induced Bronchospasm QuestionnaireZack OverfieldNoch keine Bewertungen
- 7th Semester Log BookDokument57 Seiten7th Semester Log BookaskmovieflixNoch keine Bewertungen
- Thyroid Ultrasound Preliminary EbiDokument1 SeiteThyroid Ultrasound Preliminary Ebiapi-330590877Noch keine Bewertungen
- 72423Dokument4 Seiten72423John GarzaNoch keine Bewertungen
- Ob Peds Med CardsDokument3 SeitenOb Peds Med CardsMichelle DuBose AdamsNoch keine Bewertungen
- Physical Assessment ChecklistDokument1 SeitePhysical Assessment ChecklistDMRMNoch keine Bewertungen
- Health Form OaDokument1 SeiteHealth Form OaWarren Castonguay JrNoch keine Bewertungen
- History Form IntroductoryDokument6 SeitenHistory Form Introductoryrawan.abujodahNoch keine Bewertungen
- OB PEDS Drug CardDokument3 SeitenOB PEDS Drug CardMichelle DuBose AdamsNoch keine Bewertungen
- Danbury Public Schools: Interscholastic Athletics Department Emergency Medical AuthorizationDokument1 SeiteDanbury Public Schools: Interscholastic Athletics Department Emergency Medical Authorizationapi-87536429Noch keine Bewertungen
- Medical Evaluation Form For PAPsDokument4 SeitenMedical Evaluation Form For PAPsPrint Media Printing pressNoch keine Bewertungen
- Fitness Form & Hospital ListDokument15 SeitenFitness Form & Hospital Listjohn thomasNoch keine Bewertungen
- Endoscopy Report FormatDokument1 SeiteEndoscopy Report Formatbxcrt45qkpNoch keine Bewertungen
- Health FormDokument2 SeitenHealth Formamanda6254Noch keine Bewertungen
- ConsultforElectrodiagnosticEMG FormDokument8 SeitenConsultforElectrodiagnosticEMG FormBakenaz MostafaNoch keine Bewertungen
- Blank Neurodevelopmental Intake FormDokument2 SeitenBlank Neurodevelopmental Intake FormjhecyNoch keine Bewertungen
- Referral SourceDokument10 SeitenReferral SourceHumberto FuentesNoch keine Bewertungen
- Mri Referral Package For Axxess Imaging April 2020Dokument4 SeitenMri Referral Package For Axxess Imaging April 2020JovanyGrezNoch keine Bewertungen
- Pre-Employment Health Check-Up - TPNODLDokument2 SeitenPre-Employment Health Check-Up - TPNODLBhagabati BeheraNoch keine Bewertungen
- Phone: ( - ) - Fax: ( - ) - : (Company Name) Outpatient Physical Therapy EvaluationDokument2 SeitenPhone: ( - ) - Fax: ( - ) - : (Company Name) Outpatient Physical Therapy Evaluationpt.mahmoudNoch keine Bewertungen
- URINALYSISDokument1 SeiteURINALYSISGerona Maternity Childrens ClinicNoch keine Bewertungen
- Format Pengkajian Model Doenges: Subjective (Reports)Dokument15 SeitenFormat Pengkajian Model Doenges: Subjective (Reports)mutia aNoch keine Bewertungen
- New Health and HistoryDokument3 SeitenNew Health and HistorymredubzNoch keine Bewertungen
- Gerona MaternityclinicDokument1 SeiteGerona MaternityclinicGerona Maternity Childrens ClinicNoch keine Bewertungen
- TB Chemoprophylaxis Monitor Modified 1Dokument2 SeitenTB Chemoprophylaxis Monitor Modified 1Ferry DimyatiNoch keine Bewertungen
- 10.) Medical Evaluation Form For PAPs As of 09.12.2022Dokument3 Seiten10.) Medical Evaluation Form For PAPs As of 09.12.2022SocialWelfare SilangNoch keine Bewertungen
- Complicati Ons Complicati OnsDokument2 SeitenComplicati Ons Complicati OnsTwingkol Just TwingkolNoch keine Bewertungen
- History & PE Blank ChartDokument3 SeitenHistory & PE Blank CharthellokrisjaejoongNoch keine Bewertungen
- Ac FormDokument1 SeiteAc FormLK DULLINNoch keine Bewertungen
- F.ac FormDokument1 SeiteF.ac FormRex PatambangNoch keine Bewertungen
- Gyne Assessment FormDokument8 SeitenGyne Assessment FormLal KhanNoch keine Bewertungen
- Physical Exam FormDokument1 SeitePhysical Exam FormEthan AtchleyNoch keine Bewertungen
- Cardiovascular Physiology: Review SheetDokument2 SeitenCardiovascular Physiology: Review SheetFitzHafitzNoch keine Bewertungen
- Progressive Health Care: Critical Health Care InformationVon EverandProgressive Health Care: Critical Health Care InformationNoch keine Bewertungen
- MDEH SyllabusDokument24 SeitenMDEH SyllabusAryan Singh0% (1)
- PituitaryDokument15 SeitenPituitaryBivek PokhrelNoch keine Bewertungen
- Renal FunctionDokument4 SeitenRenal FunctionCoralene Rose SilverioNoch keine Bewertungen
- The Human ConnectomeDokument9 SeitenThe Human ConnectomeSanford PepperNoch keine Bewertungen
- Anatomy of The Prostate GlandDokument18 SeitenAnatomy of The Prostate GlandRao Ghayoor DxNoch keine Bewertungen
- Lymphatic System OutlineDokument4 SeitenLymphatic System OutlineMelljonhNoch keine Bewertungen
- Classification of Joints:: Body Movements Video: Movements in Vertebrate AnimalsDokument3 SeitenClassification of Joints:: Body Movements Video: Movements in Vertebrate AnimalsThink n ExploreNoch keine Bewertungen
- Science 10 Module 2 Version 3 1Dokument17 SeitenScience 10 Module 2 Version 3 1Skyler MontalvoNoch keine Bewertungen
- Revision Notes Class 8 Science Chapter 10 - Reaching The Age of AdolescenceDokument2 SeitenRevision Notes Class 8 Science Chapter 10 - Reaching The Age of AdolescenceArpit SharmaNoch keine Bewertungen
- Anatomy and Physiology Intro.Dokument9 SeitenAnatomy and Physiology Intro.ANDREA GRAZILLE NAVAIRANoch keine Bewertungen
- Surgery Package NewDokument6 SeitenSurgery Package Newملك عيسىNoch keine Bewertungen
- Gastrointestinal Diseases Part1Dokument7 SeitenGastrointestinal Diseases Part1sarguss14100% (1)
- 2 Seminal FluidDokument10 Seiten2 Seminal FluidShyne ReyesNoch keine Bewertungen
- Thyroid Gland and Its Rule in Human BodyDokument9 SeitenThyroid Gland and Its Rule in Human BodyDrFarah Emad AliNoch keine Bewertungen
- Conduction System of The Heart PPT 2Dokument12 SeitenConduction System of The Heart PPT 2leigh angelaNoch keine Bewertungen
- Chemical Coordination and IntegrationDokument6 SeitenChemical Coordination and IntegrationRonaldNoch keine Bewertungen
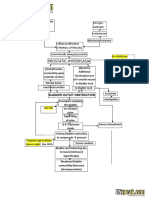
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDokument2 SeitenBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailNoch keine Bewertungen
- Physiological Control and Mechanism of Salivation: DR Oyetola Elijah Senior Lecturer/Consultant Oral Medicine, OAU/OAUTHCDokument19 SeitenPhysiological Control and Mechanism of Salivation: DR Oyetola Elijah Senior Lecturer/Consultant Oral Medicine, OAU/OAUTHCJoe AjibadeNoch keine Bewertungen
- 25 - Hungerford & Matsuda 1960Dokument630 Seiten25 - Hungerford & Matsuda 1960oséias martins magalhãesNoch keine Bewertungen
- Human ReproductionDokument35 SeitenHuman ReproductionMERYL SALOMINA FRANCISCONoch keine Bewertungen
- 3 - Tooth Morphology and Access Cavity Preparation PDFDokument6 Seiten3 - Tooth Morphology and Access Cavity Preparation PDFAhmed Al-jumailiNoch keine Bewertungen
- FELINE-Dental Radio Graphic Technique in CatsDokument7 SeitenFELINE-Dental Radio Graphic Technique in Catstaner_soysurenNoch keine Bewertungen
- Ineffective Tissue PerfusionDokument2 SeitenIneffective Tissue Perfusion8lueCzarcasmNoch keine Bewertungen
- Prepared By:: Dr. Ranjeet Kumar ChaudharyDokument22 SeitenPrepared By:: Dr. Ranjeet Kumar ChaudharyDrRanjeet Kumar ChaudharyNoch keine Bewertungen