Das könnte Ihnen auch gefallen
- Rekonstruksi SCC Dengan Flap Lateral ForeheadDokument7 SeitenRekonstruksi SCC Dengan Flap Lateral Foreheadmichaeljt_md6463Noch keine Bewertungen
- Nasal ReconstructionDokument14 SeitenNasal ReconstructionNovia Chrisnawati100% (1)
- 2010 Facial Degloving Approach To The MidfaceDokument4 Seiten2010 Facial Degloving Approach To The MidfaceAFJimenezONoch keine Bewertungen
- Plastic & Hand Surgery in Clinical Practice: Classifications and DefinitionsVon EverandPlastic & Hand Surgery in Clinical Practice: Classifications and DefinitionsNoch keine Bewertungen
- Chapter 2 The Z Plasty 2000 Fundamental Techniques of Plastic Surgery Tenth EditionDokument14 SeitenChapter 2 The Z Plasty 2000 Fundamental Techniques of Plastic Surgery Tenth Editionwerewolf3107Noch keine Bewertungen
- FlapsinplasticsurgeryDokument63 SeitenFlapsinplasticsurgerysomnathNoch keine Bewertungen
- Auric Recon Slides 070516Dokument92 SeitenAuric Recon Slides 070516Yudhistira AdeNoch keine Bewertungen
- 14 Anterolateral Thigh FlapDokument6 Seiten14 Anterolateral Thigh FlapAngga Putra100% (1)
- The Keystone Design Perforator Island Flap in Reconstructive SurgeryDokument9 SeitenThe Keystone Design Perforator Island Flap in Reconstructive SurgeryCristina Iulia100% (1)
- Oral LymphangiomaDokument8 SeitenOral LymphangiomasevattapillaiNoch keine Bewertungen
- Neligan Mandible FractureDokument17 SeitenNeligan Mandible FractureRibka TheodoraNoch keine Bewertungen
- Z Plasty - VariationsDokument7 SeitenZ Plasty - VariationsabhishekbmcNoch keine Bewertungen
- Nasolabial Flap For Oral Cavity ReconstructionDokument10 SeitenNasolabial Flap For Oral Cavity ReconstructionJamesNoch keine Bewertungen
- Flaps PDFDokument27 SeitenFlaps PDFdrgurpal74Noch keine Bewertungen
- FlapsDokument27 SeitenFlapsstegarescupavelNoch keine Bewertungen
- Flaps in Plastic Surgery by DR Roger Christopher GillDokument59 SeitenFlaps in Plastic Surgery by DR Roger Christopher GillSemi IqbalNoch keine Bewertungen
- Skin Grafts and Flaps (DR - Ricko)Dokument25 SeitenSkin Grafts and Flaps (DR - Ricko)lorensiafdNoch keine Bewertungen
- Excision of Branchial Cleft CystsDokument10 SeitenExcision of Branchial Cleft Cystssjs315Noch keine Bewertungen
- Neligan Vol 4 Chapter 10 MainDokument20 SeitenNeligan Vol 4 Chapter 10 MainisabelNoch keine Bewertungen
- Flap Plasty PDFDokument3 SeitenFlap Plasty PDFSandroNoch keine Bewertungen
- Basic Plastic Surgery Techniques and Principles: How To SutureDokument3 SeitenBasic Plastic Surgery Techniques and Principles: How To SutureDarryl BettsNoch keine Bewertungen
- Tissue Flaps: Classification and PrinciplesDokument9 SeitenTissue Flaps: Classification and PrinciplesTaufik HidayantoNoch keine Bewertungen
- Microsurgical Free FlapsDokument24 SeitenMicrosurgical Free FlapsTaufik Akbar Faried LubisNoch keine Bewertungen
- The Reconstructive LadderDokument60 SeitenThe Reconstructive Ladderterri100% (1)
- Deltopectoral FlapDokument37 SeitenDeltopectoral FlapAmbika Luthra100% (1)
- FlapDokument4 SeitenFlapMd Ahsanuzzaman PinkuNoch keine Bewertungen
- Z-Plasty For Sculpturing of The Bifid Scrotum in Severe Hypospadias Asscociated With Penoscrotal TranspositionDokument5 SeitenZ-Plasty For Sculpturing of The Bifid Scrotum in Severe Hypospadias Asscociated With Penoscrotal TranspositionneonitesNoch keine Bewertungen
- 24 Olsen Variations ParotidectomyDokument33 Seiten24 Olsen Variations ParotidectomyAngga Witra NandaNoch keine Bewertungen
- Geometry Z PlastyDokument18 SeitenGeometry Z PlastyYudi WijayaNoch keine Bewertungen
- Simple MastectomyDokument3 SeitenSimple MastectomyCindy DayocNoch keine Bewertungen
- Principles of Management of Soft Tissue SarcomaDokument33 SeitenPrinciples of Management of Soft Tissue Sarcomabashiruaminu100% (1)
- Cervicofacial LymphangiomasDokument11 SeitenCervicofacial LymphangiomasCharmila Sari100% (1)
- Advanced SuturingDokument18 SeitenAdvanced SuturingAriyanie NurtaniaNoch keine Bewertungen
- Gluteal Artery Perforator FlapsDokument8 SeitenGluteal Artery Perforator FlapsJose Mauricio Suarez BecerraNoch keine Bewertungen
- A Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryDokument9 SeitenA Novel Technique of Asian Tip Plasty by Dr. Man Koon, Suh From JW Plastic SurgeryJWPlasticsurgeryNoch keine Bewertungen
- Anterior AbdominalDokument9 SeitenAnterior AbdominalTAMBAKI EDMONDNoch keine Bewertungen
- Skin GraftsDokument25 SeitenSkin GraftsBlerina AziziNoch keine Bewertungen
- Basic Principles of Plastic SurgeryDokument46 SeitenBasic Principles of Plastic SurgeryRAJESH YADAV100% (1)
- Management of Fracture of The Edentulous Mandible Oral SurgeryDokument27 SeitenManagement of Fracture of The Edentulous Mandible Oral SurgeryFourthMolar.comNoch keine Bewertungen
- Local and Regional Flaps in Head and Neck Cancer / Orthodontic Courses by Indian Dental AcademyDokument56 SeitenLocal and Regional Flaps in Head and Neck Cancer / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- Master Degree in Plastic Surgery ThesisDokument117 SeitenMaster Degree in Plastic Surgery ThesisMohamed Ahmed El-RoubyNoch keine Bewertungen
- Congenital Infiltrating Lipomatosis of The Face Case Report PDFDokument4 SeitenCongenital Infiltrating Lipomatosis of The Face Case Report PDFfeli2010Noch keine Bewertungen
- A1 Plastic and Reconstructive Surgery - Dr. P. QuitiquitDokument7 SeitenA1 Plastic and Reconstructive Surgery - Dr. P. QuitiquitRuby Anne RomeroNoch keine Bewertungen
- Mastectomy/ Modified Radical Mastectomy: IndicationsDokument6 SeitenMastectomy/ Modified Radical Mastectomy: IndicationsNANDAN RAINoch keine Bewertungen
- Essentials CompleteDokument66 SeitenEssentials CompleteNovriman LiviaNoch keine Bewertungen
- Plastic Surgery: Understanding Abdominoplasty and LiposuctionDokument14 SeitenPlastic Surgery: Understanding Abdominoplasty and LiposuctiondoctorbanNoch keine Bewertungen
- The Five-Step Rhinoplasty Dead Space Closure TechniqueDokument2 SeitenThe Five-Step Rhinoplasty Dead Space Closure TechniqueAdRiaNa JuLIetH LoZaDa PaTiÑoNoch keine Bewertungen
- The Deltopectoral FlapDokument10 SeitenThe Deltopectoral FlapR KNoch keine Bewertungen
- Skin - Grafts by Madhuri GoreDokument112 SeitenSkin - Grafts by Madhuri GoreAnonymous 8hVpaQdCtr100% (1)
- Parotidectomy: H.Shameer AhamedDokument47 SeitenParotidectomy: H.Shameer AhamedAndreas RendraNoch keine Bewertungen
- Oncoplastic and Reconstructive BreastDokument14 SeitenOncoplastic and Reconstructive BreastYefry Onil Santana Marte100% (1)
- Cyst Neck Tumor (DR Bob Andinata)Dokument33 SeitenCyst Neck Tumor (DR Bob Andinata)Intan Eklesiana NapitupuluNoch keine Bewertungen
- Gynecomastia Surgery - Power Assisted LiposuctionDokument4 SeitenGynecomastia Surgery - Power Assisted LiposuctionAlfredo Callanta,M.D.Noch keine Bewertungen
- Keystone Flap: Kyle S. Ettinger, MD, DDS, Rui P. Fernandes, MD, DMD, FRCS (Ed), Kevin Arce, MD, DMDDokument14 SeitenKeystone Flap: Kyle S. Ettinger, MD, DDS, Rui P. Fernandes, MD, DMD, FRCS (Ed), Kevin Arce, MD, DMDlaljadeff12Noch keine Bewertungen
- 2024 Plastic Surgery - Supplementary Applicant HandbookDokument17 Seiten2024 Plastic Surgery - Supplementary Applicant HandbookwaqbinhassanNoch keine Bewertungen
- Soft Tissue SarcomaDokument45 SeitenSoft Tissue SarcomaWadhe TobingNoch keine Bewertungen
- Lecture 1 - PINCIPLES, GRAFTS & FLAPSDokument47 SeitenLecture 1 - PINCIPLES, GRAFTS & FLAPSapi-3700579100% (1)
- Alar Base Reduction and Alar-Columellar RelationshipDokument9 SeitenAlar Base Reduction and Alar-Columellar RelationshipFabian Camelo OtorrinoNoch keine Bewertungen
- Cleft Lip and Palate Management: A Comprehensive AtlasVon EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNoch keine Bewertungen
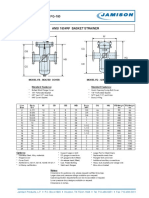
- FB-150 FQ-150 Basket StrainerDokument1 SeiteFB-150 FQ-150 Basket Strainerklich77Noch keine Bewertungen
- WDH-SL3 Iom M01M40N13-07 - 1542713324932Dokument72 SeitenWDH-SL3 Iom M01M40N13-07 - 1542713324932irwantino susilo100% (1)
- Faber, De-Ontologizing GodDokument15 SeitenFaber, De-Ontologizing GodcalfrancescoNoch keine Bewertungen
- High-Strength Stainless Steels With "Microduplex" Structure For Cryogenic ApplicationsDokument3 SeitenHigh-Strength Stainless Steels With "Microduplex" Structure For Cryogenic ApplicationsakhileshNoch keine Bewertungen
- Lecture 4: Expert Systems: What Is An Expert System?Dokument5 SeitenLecture 4: Expert Systems: What Is An Expert System?Zerihun BekeleNoch keine Bewertungen
- Manual Prevention An Control of Lost Cir PDFDokument222 SeitenManual Prevention An Control of Lost Cir PDFAna Maria TovarNoch keine Bewertungen
- Mha Mca Cet SyllabusDokument20 SeitenMha Mca Cet Syllabusm kumarNoch keine Bewertungen
- Chapter 11Dokument53 SeitenChapter 11Vijendhar ReddyNoch keine Bewertungen
- Reliability Analysis Center: Practical Considerations in Calculating Reliability of Fielded ProductsDokument24 SeitenReliability Analysis Center: Practical Considerations in Calculating Reliability of Fielded ProductsNg Wei LihNoch keine Bewertungen
- Inform: Extending PhoenicsDokument42 SeitenInform: Extending PhoenicsrsigorNoch keine Bewertungen
- Sentiment AnalysisDokument5 SeitenSentiment AnalysisShruti PantNoch keine Bewertungen
- Postmodernity in PiDokument2 SeitenPostmodernity in Pixhardy27Noch keine Bewertungen
- Camshaft Recommendation FormDokument3 SeitenCamshaft Recommendation Formcrower_scribdNoch keine Bewertungen
- 3DC Real Light 24HDRi Vol03Dokument27 Seiten3DC Real Light 24HDRi Vol03AntezanaFernandoNoch keine Bewertungen
- Proportional Directional Valves: Series LVS08 and LVS12 - Preferred Products ProgrammeDokument66 SeitenProportional Directional Valves: Series LVS08 and LVS12 - Preferred Products ProgrammealeksandrNoch keine Bewertungen
- Pedestrian Safety AnalysisDokument12 SeitenPedestrian Safety Analysispartha sreekarNoch keine Bewertungen
- 351 DatasheetDokument14 Seiten351 DatasheetRafael NavarroNoch keine Bewertungen
- TFT SDK ManualDokument107 SeitenTFT SDK ManualRenier ServenNoch keine Bewertungen
- Regression Analysis AssignmentDokument8 SeitenRegression Analysis Assignmentضیاء گل مروت100% (1)
- Netxknx Opc 3 - 5 - 4 EngDokument93 SeitenNetxknx Opc 3 - 5 - 4 Engtai_sao_khong_1307Noch keine Bewertungen
- Maths Shortcuts by DayTodayGKDokument20 SeitenMaths Shortcuts by DayTodayGKAnand KesarkarNoch keine Bewertungen
- Upcoming: Advisor Webcast: Oracle Database Resource ManagerDokument41 SeitenUpcoming: Advisor Webcast: Oracle Database Resource ManagerLayne MoránNoch keine Bewertungen
- Grade 9 Cells and Cell Movements Formative WorksheetDokument8 SeitenGrade 9 Cells and Cell Movements Formative WorksheetHari PatelNoch keine Bewertungen
- XML SerializationDokument4 SeitenXML Serializationapi-3748960Noch keine Bewertungen
- SMO Senior 2017Dokument6 SeitenSMO Senior 2017Kanchit SaehoNoch keine Bewertungen
- Engineering Properties of Soil PDFDokument55 SeitenEngineering Properties of Soil PDFJam Apizara Chaizalee100% (1)
- Beration of LightDokument7 SeitenBeration of LightAnonymous i71HvPXNoch keine Bewertungen
- Analytic Geometry Parabola ProblemsDokument14 SeitenAnalytic Geometry Parabola ProblemsOjit QuizonNoch keine Bewertungen
- 截屏 2021-08-05 17.02.20Dokument98 Seiten截屏 2021-08-05 17.02.204WEM GTNoch keine Bewertungen
- What Is Lincdoc?Dokument2 SeitenWhat Is Lincdoc?Daniel O'Leary0% (1)