Das könnte Ihnen auch gefallen
- Writing White PapersDokument194 SeitenWriting White PapersPrasannaYalamanchili80% (5)
- Doconnell - Catholic Health Care Ministries ReflecitonDokument4 SeitenDoconnell - Catholic Health Care Ministries Reflecitonapi-356132267Noch keine Bewertungen
- Already Missional: Congregations as Community PartnersVon EverandAlready Missional: Congregations as Community PartnersNoch keine Bewertungen
- When Helping Hurts: The Small Group Experience: An Online Video-Based Study on Alleviating PovertyVon EverandWhen Helping Hurts: The Small Group Experience: An Online Video-Based Study on Alleviating PovertyBewertung: 5 von 5 Sternen5/5 (1)
- FBL ManualDokument12 SeitenFBL Manualaurumstar2000Noch keine Bewertungen
- Smaller Churches Have at Least Five AdvantagesDokument5 SeitenSmaller Churches Have at Least Five AdvantagesMatthew LopezNoch keine Bewertungen
- The Let My People Go Handbook: Equipping Your Church to Love Those Most VulnerableVon EverandThe Let My People Go Handbook: Equipping Your Church to Love Those Most VulnerableNoch keine Bewertungen
- 5 Claves A Mantener en El Ministerio.Dokument7 Seiten5 Claves A Mantener en El Ministerio.juanNoch keine Bewertungen
- Taking Action A Parish Strategy For Legislative AdvocacyDokument53 SeitenTaking Action A Parish Strategy For Legislative AdvocacyCCUSA_PSMNoch keine Bewertungen
- Glad Tidings: "New Year's Revolutions"Dokument8 SeitenGlad Tidings: "New Year's Revolutions"centralstmatthewuccNoch keine Bewertungen
- Faith-Based Organisations and Responses To Displacement FMRDokument3 SeitenFaith-Based Organisations and Responses To Displacement FMRiihaoutreachNoch keine Bewertungen
- Christianity and the Mega Church: Soul Winning or Competitive BusinessVon EverandChristianity and the Mega Church: Soul Winning or Competitive BusinessNoch keine Bewertungen
- September Newsletter 2018-FinalDokument10 SeitenSeptember Newsletter 2018-Finalapi-329478828Noch keine Bewertungen
- Grab, Gather, Grow: Multiply Community Groups in Your ChurchVon EverandGrab, Gather, Grow: Multiply Community Groups in Your ChurchNoch keine Bewertungen
- Surviving a Bad Economy: Biblical Principles for Success in Any EconomyVon EverandSurviving a Bad Economy: Biblical Principles for Success in Any EconomyNoch keine Bewertungen
- Faith-Based Organizing: A Congregational Planning Resource for Addressing PovertyVon EverandFaith-Based Organizing: A Congregational Planning Resource for Addressing PovertyNoch keine Bewertungen
- 9 Lies Most Churches Abide byDokument3 Seiten9 Lies Most Churches Abide byapi-25949894Noch keine Bewertungen
- The Other 80 Percent: Turning Your Church's Spectators into Active ParticipantsVon EverandThe Other 80 Percent: Turning Your Church's Spectators into Active ParticipantsNoch keine Bewertungen
- The Sissi Principles: Sales, Investments, Salaries, Services and InheritancesVon EverandThe Sissi Principles: Sales, Investments, Salaries, Services and InheritancesNoch keine Bewertungen
- Intervention in Church Conflict: A Narrative-Systems ApproachVon EverandIntervention in Church Conflict: A Narrative-Systems ApproachNoch keine Bewertungen
- The Effectiveness of Church-Based Prosperity Programs: Findings of an Exploratory StudyVon EverandThe Effectiveness of Church-Based Prosperity Programs: Findings of an Exploratory StudyNoch keine Bewertungen
- Reflection Again Dconclusion Nalang at Final EditDokument4 SeitenReflection Again Dconclusion Nalang at Final EditAyejae PateñaNoch keine Bewertungen
- 17 Feb PDFDokument19 Seiten17 Feb PDFMarciaMccormickNoch keine Bewertungen
- CurriculumDokument52 SeitenCurriculumTOPS LUKAMBONoch keine Bewertungen
- 12 Steps To Starting A CMCDokument22 Seiten12 Steps To Starting A CMCChanel ANoch keine Bewertungen
- Ideas Regarding Church MergersDokument4 SeitenIdeas Regarding Church Mergerseasygoing1Noch keine Bewertungen
- Trending Up: Social Media Strategies for Today's ChurchVon EverandTrending Up: Social Media Strategies for Today's ChurchBewertung: 5 von 5 Sternen5/5 (2)
- The Influence Course: Your Journey into God's Heart for Good GovernanceVon EverandThe Influence Course: Your Journey into God's Heart for Good GovernanceNoch keine Bewertungen
- The Vile Practices of Church Leadership: Finance and AdministrationVon EverandThe Vile Practices of Church Leadership: Finance and AdministrationNoch keine Bewertungen
- The Unique Role of The Local Church in Developing A Flourishing Community VogtDokument9 SeitenThe Unique Role of The Local Church in Developing A Flourishing Community VogtWalben SijabatNoch keine Bewertungen
- Toolkit PrompangDokument13 SeitenToolkit PrompangpabloNoch keine Bewertungen
- CS-NW 2014 Narrative v1.7Dokument7 SeitenCS-NW 2014 Narrative v1.7Regent BrownNoch keine Bewertungen
- A Manual On Lay FormationDokument23 SeitenA Manual On Lay FormationMelvin JacintoNoch keine Bewertungen
- Out of Poverty March 2014Dokument15 SeitenOut of Poverty March 2014api-247412182Noch keine Bewertungen
- Alternative Financial Models For Churches and Church Plants: When Tithes and Offerings Are Not EnoughDokument23 SeitenAlternative Financial Models For Churches and Church Plants: When Tithes and Offerings Are Not EnoughtahangNoch keine Bewertungen
- Supply Lines: Five Supporting Relationships Every Planter and Pastor NeedsVon EverandSupply Lines: Five Supporting Relationships Every Planter and Pastor NeedsNoch keine Bewertungen
- 3 Solidarity and ResponsibilityDokument6 Seiten3 Solidarity and Responsibilitykwintencirkel3715Noch keine Bewertungen
- The Caring Congregation Ministry Implementation Guide: Implementation GuideVon EverandThe Caring Congregation Ministry Implementation Guide: Implementation GuideNoch keine Bewertungen
- Coloso, Dakki Lindo, Ysh Moreno, Stephanie NG, Victor Oshikawa, HiroDokument17 SeitenColoso, Dakki Lindo, Ysh Moreno, Stephanie NG, Victor Oshikawa, Hirohiro_oshikawa7961Noch keine Bewertungen
- Back to Zero: The Search to Rediscover the Methodist MovementVon EverandBack to Zero: The Search to Rediscover the Methodist MovementBewertung: 2.5 von 5 Sternen2.5/5 (5)
- ST Daniels Digitalmedia ReportDokument9 SeitenST Daniels Digitalmedia Reportapi-138229013Noch keine Bewertungen
- Family Activism: Empowering Your Community, Beginning with Family and FriendsVon EverandFamily Activism: Empowering Your Community, Beginning with Family and FriendsNoch keine Bewertungen
- Reed 4 - Enabling AssessmentDokument2 SeitenReed 4 - Enabling AssessmentCryslerNoch keine Bewertungen
- Congressional Testimony - Patrick Raglow, Oklahoma City - House Agriculture CommitteeDokument7 SeitenCongressional Testimony - Patrick Raglow, Oklahoma City - House Agriculture CommitteeCatholic Charities USANoch keine Bewertungen
- Strengths and Weaknesses of American Churches PreprintDokument15 SeitenStrengths and Weaknesses of American Churches PreprintJonahNoch keine Bewertungen
- PAPER On POORDokument6 SeitenPAPER On POORRoger Ryan AlbaNoch keine Bewertungen
- Criterion-Institute-Blueprint FaithBased Organizations 033021Dokument51 SeitenCriterion-Institute-Blueprint FaithBased Organizations 033021Blackw JeffNoch keine Bewertungen
- Connecting the Dots: Ministering to Your Congregation Through Its Organizational SystemVon EverandConnecting the Dots: Ministering to Your Congregation Through Its Organizational SystemNoch keine Bewertungen
- Preparation For The General Chapter 2019Dokument6 SeitenPreparation For The General Chapter 2019BlimpNoch keine Bewertungen
- ActivityDokument2 SeitenActivityMaxine RicafortNoch keine Bewertungen
- Senior Sensitive MinistryDokument4 SeitenSenior Sensitive MinistryEbri OjeNoch keine Bewertungen
- Becoming One: Volume 2 The Diversity Salad Bowl Open MindVon EverandBecoming One: Volume 2 The Diversity Salad Bowl Open MindNoch keine Bewertungen
- Purpose Driven CampaigningDokument14 SeitenPurpose Driven CampaigningAlex StevensNoch keine Bewertungen
- Mission and VisionDokument1 SeiteMission and VisionVirginia MCNoch keine Bewertungen
- Leadership Resources 2012-13Dokument1 SeiteLeadership Resources 2012-13Virginia MCNoch keine Bewertungen
- Constitution & Bylaws 2012Dokument15 SeitenConstitution & Bylaws 2012Virginia MCNoch keine Bewertungen
- Spouse Response Form TypeableDokument2 SeitenSpouse Response Form TypeableVirginia MCNoch keine Bewertungen
- Where I'm From PoemDokument1 SeiteWhere I'm From PoemVirginia MCNoch keine Bewertungen
- Seven Vision StatementsDokument1 SeiteSeven Vision StatementsVirginia MCNoch keine Bewertungen
- MTTF ApplicationDokument2 SeitenMTTF ApplicationVirginia MC100% (2)
- Credentialing For Ministry Journey (Outline)Dokument4 SeitenCredentialing For Ministry Journey (Outline)Virginia MCNoch keine Bewertungen
- Credentialing For Ministry Journey (With Attachments)Dokument15 SeitenCredentialing For Ministry Journey (With Attachments)Virginia MCNoch keine Bewertungen
- Growing in Ministry Journey (Outline)Dokument4 SeitenGrowing in Ministry Journey (Outline)Virginia MCNoch keine Bewertungen
- Quarterly ReportDokument2 SeitenQuarterly ReportVirginia MCNoch keine Bewertungen
- Resources For The JourneyDokument4 SeitenResources For The JourneyVirginia MCNoch keine Bewertungen
- Special Ministries PolicyDokument4 SeitenSpecial Ministries PolicyVirginia MCNoch keine Bewertungen
- I.Congregational Polity: The Nature and Mission of The ChurchDokument40 SeitenI.Congregational Polity: The Nature and Mission of The ChurchVirginia MCNoch keine Bewertungen
- Organizational ChartDokument1 SeiteOrganizational ChartVirginia MCNoch keine Bewertungen
- Virginia Mennonite Conference: Ministerial Candidate Response Form Information Sheet For Personnel CommitteeDokument1 SeiteVirginia Mennonite Conference: Ministerial Candidate Response Form Information Sheet For Personnel CommitteeVirginia MCNoch keine Bewertungen
- Agreeing and Disagreeing in LoveDokument2 SeitenAgreeing and Disagreeing in LoveVirginia MCNoch keine Bewertungen
- Personnel Committee QuestionnaireDokument2 SeitenPersonnel Committee QuestionnaireVirginia MCNoch keine Bewertungen
- Business and Finance TerminologyDokument15 SeitenBusiness and Finance TerminologyKat KatNoch keine Bewertungen
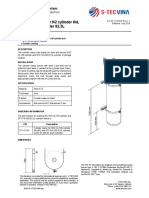
- Cylinder Clamp For N2 Cylinder 84L and FM-200 Cylinder 82.5LDokument1 SeiteCylinder Clamp For N2 Cylinder 84L and FM-200 Cylinder 82.5LNguyễn Minh ThiệuNoch keine Bewertungen
- Brochure PVM enDokument36 SeitenBrochure PVM enBenny Kurniawan LimNoch keine Bewertungen
- SANAKO Study700 V 500 BrochureDokument4 SeitenSANAKO Study700 V 500 BrochureDwi PrihantoroNoch keine Bewertungen
- Boarding PassDokument1 SeiteBoarding PassFajarNoch keine Bewertungen
- BrochureDokument8 SeitenBrochurevacmanilaNoch keine Bewertungen
- BioEdit Version 7.0.0 PDFDokument192 SeitenBioEdit Version 7.0.0 PDFJovanderson JacksonNoch keine Bewertungen
- Ranbaxy Acquisition by DaiichiDokument9 SeitenRanbaxy Acquisition by Daiichirupe59Noch keine Bewertungen
- Virtual Asset Insurance Risk Analysis - OneDegreeDokument3 SeitenVirtual Asset Insurance Risk Analysis - OneDegreeShaarang BeganiNoch keine Bewertungen
- Jurnal Stamina: E-ISSN 2655-2515 P-ISSN 2655-1802Dokument9 SeitenJurnal Stamina: E-ISSN 2655-2515 P-ISSN 2655-1802Yogi TioNoch keine Bewertungen
- SDS enDokument6 SeitenSDS enAnup BajracharyaNoch keine Bewertungen
- Honeywell Aquatrol 2000 PDFDokument60 SeitenHoneywell Aquatrol 2000 PDFvsilickasNoch keine Bewertungen
- FII Ordering SuppliesDokument9 SeitenFII Ordering SuppliesO GamezNoch keine Bewertungen
- IMO - PowerpointDokument16 SeitenIMO - PowerpointMahen Fernando100% (3)
- Guide To Manually Importing/Transferring Your Livery For FH4/FM7/FH3 PCDokument12 SeitenGuide To Manually Importing/Transferring Your Livery For FH4/FM7/FH3 PCLennike SantosNoch keine Bewertungen
- Teit Cbgs Dmbi Lab Manual FH 2015Dokument60 SeitenTeit Cbgs Dmbi Lab Manual FH 2015Soumya PandeyNoch keine Bewertungen
- Soal Ujian SmaDokument26 SeitenSoal Ujian SmaAyu RiskyNoch keine Bewertungen
- Editing Packs I Maybe Will NeedDokument3 SeitenEditing Packs I Maybe Will NeedMijo SusićNoch keine Bewertungen
- RMU With Eco-Efficient Gas Mixture-Evaluation After Three Years of Field ExperienceDokument5 SeitenRMU With Eco-Efficient Gas Mixture-Evaluation After Three Years of Field ExperienceZineddine BENOUADAHNoch keine Bewertungen
- NO.76 Method Statement for Chemical Anchoring of Rebars on Piles - Rev.0第一次Dokument5 SeitenNO.76 Method Statement for Chemical Anchoring of Rebars on Piles - Rev.0第一次Amila Priyadarshana DissanayakeNoch keine Bewertungen
- Eligibility To Become IAS Officer: Career As A IAS Officer About IAS OfficerDokument4 SeitenEligibility To Become IAS Officer: Career As A IAS Officer About IAS Officersamiie30Noch keine Bewertungen
- PDF Applied Failure Analysis 1 NSW - CompressDokument2 SeitenPDF Applied Failure Analysis 1 NSW - CompressAgungNoch keine Bewertungen
- Canon IR2016J Error Code ListDokument4 SeitenCanon IR2016J Error Code ListZahidShaikhNoch keine Bewertungen
- Remedial Law Syllabus 2013Dokument6 SeitenRemedial Law Syllabus 2013Mirriam Ebreo100% (1)
- Midterm Fin Oo4Dokument82 SeitenMidterm Fin Oo4patricia gunio100% (1)
- International Advertising: Definition of International MarketingDokument2 SeitenInternational Advertising: Definition of International MarketingAfad KhanNoch keine Bewertungen
- Electronics World 1962 11Dokument114 SeitenElectronics World 1962 11meisterwantNoch keine Bewertungen
- A Study On Impact of Acne Vulgaris On Quality of LifeDokument7 SeitenA Study On Impact of Acne Vulgaris On Quality of LifeIJAR JOURNALNoch keine Bewertungen