Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
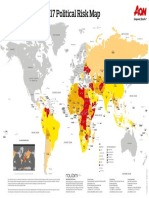
- Political Risk Map 2017Dokument1 SeitePolitical Risk Map 2017Mahesh ParabNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Visual Basics For ApplicationsDokument141 SeitenVisual Basics For ApplicationsMahesh ParabNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- NetworkingDokument104 SeitenNetworkingMahesh ParabNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- ICICI Lombard Project ReportDokument91 SeitenICICI Lombard Project ReportMahesh Parab75% (4)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- C Class AssignmentsDokument65 SeitenC Class AssignmentsMahesh ParabNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Insurance ProjDokument20 SeitenInsurance ProjMahesh ParabNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- PAKKAMDokument4 SeitenPAKKAM267083Noch keine Bewertungen
- Restaurant Opening ChecklistDokument47 SeitenRestaurant Opening ChecklistAssemNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- TN HP ActDokument2 SeitenTN HP ActSiddharth BhandariNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Tacn1 HVTCDokument9 SeitenTacn1 HVTCNgô Khánh HuyềnNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Cost Estimation PDFDokument16 SeitenCost Estimation PDFemadsabriNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Bitcoin Halving, Explained: Mar 24, 2020updated Apr 6, 2020Dokument11 SeitenBitcoin Halving, Explained: Mar 24, 2020updated Apr 6, 2020Pieter SteenkampNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- đề 1 kinh tế học tài chính 1Dokument12 Seitenđề 1 kinh tế học tài chính 1Hùng PhanNoch keine Bewertungen
- KYCDokument2 SeitenKYCRamkumarNoch keine Bewertungen
- Case Study: Crowdfunding KENYA: Aidana Koshenova Sarah Nesrala Melvin Carrasquillo Felman Antonio Ruiz RodriguezDokument13 SeitenCase Study: Crowdfunding KENYA: Aidana Koshenova Sarah Nesrala Melvin Carrasquillo Felman Antonio Ruiz RodriguezAhmed El KhateebNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- London Metal Exchange - LME CopperDokument1 SeiteLondon Metal Exchange - LME CopperRehan SadiqNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Dwnload Full Advanced Accounting 12th Edition Fischer Test Bank PDFDokument35 SeitenDwnload Full Advanced Accounting 12th Edition Fischer Test Bank PDFunrudesquirtjghzl100% (14)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Lump Sum LiquidationDokument4 SeitenLump Sum LiquidationKara Manansala LayuganNoch keine Bewertungen
- Calamos Market Neutral Income Fund: CmnixDokument2 SeitenCalamos Market Neutral Income Fund: CmnixAl BruceNoch keine Bewertungen
- FN2029 - FI - 2011 Examiners Commentaries - Zone-BDokument8 SeitenFN2029 - FI - 2011 Examiners Commentaries - Zone-BScarlett Ford GeronimoNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Memorandum Articles of Association enDokument24 SeitenMemorandum Articles of Association enrahmajdNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Initiating Coverage On JP Associates LTDDokument23 SeitenInitiating Coverage On JP Associates LTDVarun YadavNoch keine Bewertungen
- Licensing of Credit Reference BureauDokument4 SeitenLicensing of Credit Reference BureauKofikoduahNoch keine Bewertungen
- Cost of Capital Project PDFDokument50 SeitenCost of Capital Project PDFPreet PreetNoch keine Bewertungen
- Forecasting Financial StatementsDokument58 SeitenForecasting Financial StatementsEman KhalilNoch keine Bewertungen
- Business Mathematics: For LearnersDokument13 SeitenBusiness Mathematics: For LearnersJet Rollorata BacangNoch keine Bewertungen
- Fixedline and Broadband Services: Your Account Summary This Month'S ChargesDokument3 SeitenFixedline and Broadband Services: Your Account Summary This Month'S ChargesLalit SharmaNoch keine Bewertungen
- Fundamentals of Venture Capital (PDFDrive)Dokument162 SeitenFundamentals of Venture Capital (PDFDrive)Boboy AzanilNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Exercise 4 MAKE A PIVOT TABLEDokument4 SeitenExercise 4 MAKE A PIVOT TABLEMoonchaserNoch keine Bewertungen
- Case 4. Morgan Stanley and The Market RiskDokument8 SeitenCase 4. Morgan Stanley and The Market RiskJakeNoch keine Bewertungen
- Field Verification Proforma For DR - YSR Aarogyasri Health CardDokument1 SeiteField Verification Proforma For DR - YSR Aarogyasri Health Cardjegurupadu gpNoch keine Bewertungen
- Consultant Application Form BookDokument2 SeitenConsultant Application Form Bookhetalben bhatt100% (1)
- New Rekening Koran Online 493501004332535 2023-02-01 2023-02-28 00326282 PDFDokument2 SeitenNew Rekening Koran Online 493501004332535 2023-02-01 2023-02-28 00326282 PDFSupebriasa AmdNoch keine Bewertungen
- Final Project ForexDokument145 SeitenFinal Project ForexdamupatelNoch keine Bewertungen
- Succession ApplicationDokument220 SeitenSuccession ApplicationRaja Khan50% (2)
- IAS16Dokument18 SeitenIAS16Peter, DeogratiasNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)