Das könnte Ihnen auch gefallen
- Assistant Attorney General Matt Hartman's RulingDokument7 SeitenAssistant Attorney General Matt Hartman's RulingsaukvalleynewsNoch keine Bewertungen
- Potential: SolutionsDokument15 SeitenPotential: SolutionssaukvalleynewsNoch keine Bewertungen
- Reyes PetitionDokument1 SeiteReyes PetitionsaukvalleynewsNoch keine Bewertungen
- Dixon CBA 2016 2020 FinalDokument48 SeitenDixon CBA 2016 2020 FinalsaukvalleynewsNoch keine Bewertungen
- Erie CES1 4-26-16 Part III PDFDokument14 SeitenErie CES1 4-26-16 Part III PDFsaukvalleynewsNoch keine Bewertungen
- 2016 Income Eligibility GuidelinesDokument1 Seite2016 Income Eligibility GuidelinessaukvalleynewsNoch keine Bewertungen
- Erie CES1 4-26-16 Part II PDFDokument12 SeitenErie CES1 4-26-16 Part II PDFsaukvalleynewsNoch keine Bewertungen
- Erie CES1 4-26-16 Part IDokument14 SeitenErie CES1 4-26-16 Part IsaukvalleynewsNoch keine Bewertungen
- Rock Falls Drug ConspiracyDokument7 SeitenRock Falls Drug ConspiracysaukvalleynewsNoch keine Bewertungen
- Notes From Charrette Map 2Dokument1 SeiteNotes From Charrette Map 2saukvalleynewsNoch keine Bewertungen
- Erie Facilities Plan PresentationDokument55 SeitenErie Facilities Plan PresentationsaukvalleynewsNoch keine Bewertungen
- New Officer AgreementDokument2 SeitenNew Officer AgreementsaukvalleynewsNoch keine Bewertungen
- Park Map For FarmapaloozaDokument1 SeitePark Map For FarmapaloozasaukvalleynewsNoch keine Bewertungen
- Notes From Charrette Map 3Dokument1 SeiteNotes From Charrette Map 3saukvalleynewsNoch keine Bewertungen
- Notes From Charrette Map 1Dokument1 SeiteNotes From Charrette Map 1saukvalleynewsNoch keine Bewertungen
- Education Foundation Scholarhsip - 2016Dokument3 SeitenEducation Foundation Scholarhsip - 2016saukvalleynewsNoch keine Bewertungen
- Table 2Dokument1 SeiteTable 2saukvalleynewsNoch keine Bewertungen
- Notes From Charrette Map 1 3Dokument1 SeiteNotes From Charrette Map 1 3saukvalleynewsNoch keine Bewertungen
- Notes From Charrette Map 3Dokument1 SeiteNotes From Charrette Map 3saukvalleynewsNoch keine Bewertungen
- Notes From Charrette Map 2Dokument1 SeiteNotes From Charrette Map 2saukvalleynewsNoch keine Bewertungen
- Education Foundation Grant Program - Donald Hill-2016Dokument3 SeitenEducation Foundation Grant Program - Donald Hill-2016saukvalleynewsNoch keine Bewertungen
- AGclubflyer W LocationDokument1 SeiteAGclubflyer W LocationsaukvalleynewsNoch keine Bewertungen
- Morrison Police Sergeant Job DescriptionDokument44 SeitenMorrison Police Sergeant Job DescriptionsaukvalleynewsNoch keine Bewertungen
- Lee County Jail - PresentationDokument18 SeitenLee County Jail - PresentationsaukvalleynewsNoch keine Bewertungen
- MIA Tour BreakdownDokument5 SeitenMIA Tour BreakdownsaukvalleynewsNoch keine Bewertungen
- Doubles Pickleball Round Robin 031216 2Dokument2 SeitenDoubles Pickleball Round Robin 031216 2saukvalleynewsNoch keine Bewertungen
- Allensworth & Easton (2007)Dokument68 SeitenAllensworth & Easton (2007)saukvalleynewsNoch keine Bewertungen
- ICTM Regional CompetitionDokument6 SeitenICTM Regional CompetitionsaukvalleynewsNoch keine Bewertungen
- City of Dixon Recovered FundsDokument1 SeiteCity of Dixon Recovered FundssaukvalleynewsNoch keine Bewertungen
- Exhibit BDokument19 SeitenExhibit BsaukvalleynewsNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Extent of Liability Imposed by The Warsaw Convention On International Air CarriersDokument4 SeitenThe Extent of Liability Imposed by The Warsaw Convention On International Air CarriersnashNoch keine Bewertungen
- Case Digest PALEDokument31 SeitenCase Digest PALEEve Salt100% (1)
- Abakada Vs ErmitaDokument2 SeitenAbakada Vs ErmitaCarlota Nicolas VillaromanNoch keine Bewertungen
- PHL-InD - The Indonesian Diaspora and Philippine-Indonesian RelationsDokument14 SeitenPHL-InD - The Indonesian Diaspora and Philippine-Indonesian RelationsFrancesca Dominique C. JimenezNoch keine Bewertungen
- Speech OutlineDokument7 SeitenSpeech OutlineDmitryNoch keine Bewertungen
- Data Kehadiran Murid HSN 2016Dokument27 SeitenData Kehadiran Murid HSN 2016MOHD NAZRI BIN ZAKARIA KPM-GuruNoch keine Bewertungen
- Football P.E.Dokument5 SeitenFootball P.E.Amanda MohammedNoch keine Bewertungen
- How I Messed Up Meeting My Girlfriend's ParentsDokument2 SeitenHow I Messed Up Meeting My Girlfriend's ParentsCikgu ShimaNoch keine Bewertungen
- Atty Torres DisbarredDokument3 SeitenAtty Torres DisbarredJanet Tal-udanNoch keine Bewertungen
- Republic vs. Kho: Compliance with Rule 108 allows correction of substantial errors in civil registryDokument2 SeitenRepublic vs. Kho: Compliance with Rule 108 allows correction of substantial errors in civil registryLorenzo Angelo OcampoNoch keine Bewertungen
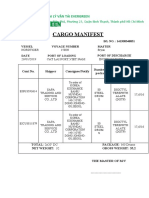
- Cargo Manifest: Công Ty Tnhh Đại Lý Vận Tải EvergreenDokument2 SeitenCargo Manifest: Công Ty Tnhh Đại Lý Vận Tải EvergreenFeng KrissNoch keine Bewertungen
- CLJ 3 - Lecture 1Dokument22 SeitenCLJ 3 - Lecture 1Euben PatronNoch keine Bewertungen
- Notes - Constitutional Law 2 (Police Power) Digested-1Dokument121 SeitenNotes - Constitutional Law 2 (Police Power) Digested-1Fred AbisNoch keine Bewertungen
- Self Exam HumilityDokument3 SeitenSelf Exam HumilityAndrew Mitry100% (14)
- Reported Speech WorksheetDokument3 SeitenReported Speech WorksheetPABLO POSADA COLORADONoch keine Bewertungen
- History of IPRADokument16 SeitenHistory of IPRASharmin ReulaNoch keine Bewertungen
- Strat Acitvity TodayDokument1 SeiteStrat Acitvity TodayJosiah Vino100% (2)
- Types of StatutesDokument12 SeitenTypes of StatutesShubham PandeyNoch keine Bewertungen
- Osg V. Ayala Land IncDokument23 SeitenOsg V. Ayala Land IncGLORILYN MONTEJONoch keine Bewertungen
- Curtain Poirots Last CaseDokument34 SeitenCurtain Poirots Last CaseRiya GuptaNoch keine Bewertungen
- Lupo Atienza v. Judge Brilliantes PDFDokument6 SeitenLupo Atienza v. Judge Brilliantes PDFchescasenNoch keine Bewertungen
- Unbroken Soldier (Storm of Duster)Dokument76 SeitenUnbroken Soldier (Storm of Duster)ignorantorange100% (1)
- Obg Icd-10 Pregnancy, Childbirth, PuerperiumDokument11 SeitenObg Icd-10 Pregnancy, Childbirth, PuerperiumarifianjuariNoch keine Bewertungen
- Introduction To Private International LawDokument9 SeitenIntroduction To Private International LawŤşinu MđNoch keine Bewertungen
- Essay 2 Psyc 4p71Dokument14 SeitenEssay 2 Psyc 4p71api-534375900Noch keine Bewertungen
- PD 223Dokument4 SeitenPD 223Catly CapistranoNoch keine Bewertungen
- BIO Ethics ApprovalDokument10 SeitenBIO Ethics ApprovalandrewperezdcNoch keine Bewertungen
- Top 40 love songs for weddingsDokument10 SeitenTop 40 love songs for weddingsyanachii22Noch keine Bewertungen
- Konseling Traumatik Pendekatan Cognitif-Behavior Therapy: Etty SetiawatiDokument16 SeitenKonseling Traumatik Pendekatan Cognitif-Behavior Therapy: Etty SetiawatiGilang AnandaNoch keine Bewertungen
- Negotiable Instruments Timoteo AquinoDokument328 SeitenNegotiable Instruments Timoteo AquinoAntonio Santos88% (34)