Das könnte Ihnen auch gefallen
- Medicaid AppealDokument15 SeitenMedicaid Appealmtp7389Noch keine Bewertungen
- New Patient Reg FormDokument7 SeitenNew Patient Reg FormDr.HunanyanNoch keine Bewertungen
- Bpacnz Antibiotics GuideDokument40 SeitenBpacnz Antibiotics GuideBulborea MihaelaNoch keine Bewertungen
- Patient Registration Form: General Information (Please Print Neatly)Dokument5 SeitenPatient Registration Form: General Information (Please Print Neatly)Dan ThomasNoch keine Bewertungen
- Patient Registration Form 13Dokument4 SeitenPatient Registration Form 13windawaty humolaNoch keine Bewertungen
- Patient Information and Benefits Assignment & ReleaseDokument17 SeitenPatient Information and Benefits Assignment & ReleaseMr. Alma Myers, LAcNoch keine Bewertungen
- Patient Information Sheet 091409Dokument2 SeitenPatient Information Sheet 091409api-16816262Noch keine Bewertungen
- Cross-Training: The Medical Assistant WorkbookVon EverandCross-Training: The Medical Assistant WorkbookNoch keine Bewertungen
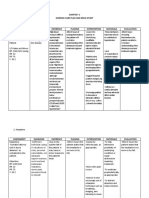
- NCP For Dizziness and HeadacheDokument4 SeitenNCP For Dizziness and Headachekarthi karthi100% (1)
- Essential GCP by Prof David Hutchinson 2017Dokument78 SeitenEssential GCP by Prof David Hutchinson 2017Luis Marcas VilaNoch keine Bewertungen
- Logo New Patient Packet 2016Dokument4 SeitenLogo New Patient Packet 2016api-283388825Noch keine Bewertungen
- Burnout in CounselingDokument54 SeitenBurnout in CounselingmokaNoch keine Bewertungen
- Report 8b3a3101Dokument11 SeitenReport 8b3a3101Pooja AgarwalNoch keine Bewertungen
- Kaiser Volunteer ApplicationDokument6 SeitenKaiser Volunteer ApplicationVanessa HoNoch keine Bewertungen
- Memorial Hermann Discharge Papers - 3Dokument5 SeitenMemorial Hermann Discharge Papers - 3Alaska JamesNoch keine Bewertungen
- Acupuncture Intake FormDokument2 SeitenAcupuncture Intake FormMeraki MaryNoch keine Bewertungen
- 1st Term .Jss3 PheDokument17 Seiten1st Term .Jss3 Phesamuel joshuaNoch keine Bewertungen
- Observership ApplicationDokument3 SeitenObservership ApplicationMatheus AzevedoNoch keine Bewertungen
- NP Paperwork 2018Dokument7 SeitenNP Paperwork 2018api-246819968Noch keine Bewertungen
- Male New Patient Paperwork 5.2015Dokument8 SeitenMale New Patient Paperwork 5.2015Muhammad AdeelNoch keine Bewertungen
- New Patient Package 2021 ICARE RXDokument15 SeitenNew Patient Package 2021 ICARE RXAckie LoyolaNoch keine Bewertungen
- Initial Client Paperwork 1-16Dokument5 SeitenInitial Client Paperwork 1-16api-272512227Noch keine Bewertungen
- Pde 294Dokument6 SeitenPde 294marcusscoobyNoch keine Bewertungen
- MedicalVerification PDFDokument3 SeitenMedicalVerification PDFOptical RecoveryNoch keine Bewertungen
- Cooperative Health Management Federation: Enrollment Application Form (Eaf)Dokument2 SeitenCooperative Health Management Federation: Enrollment Application Form (Eaf)Geraldine Daquipil TortalNoch keine Bewertungen
- Family Application Form: Please Print ClearlyDokument9 SeitenFamily Application Form: Please Print ClearlyJulie Lyles CarrNoch keine Bewertungen
- Practice of Chet Gentry, MD Alison Hicks, FNP-C Tiffany Ward, FNP-BC William Wilson, FNPDokument6 SeitenPractice of Chet Gentry, MD Alison Hicks, FNP-C Tiffany Ward, FNP-BC William Wilson, FNPPeyton BooherNoch keine Bewertungen
- PATIENT INFORMATION - Please Fill Out CompletelyDokument5 SeitenPATIENT INFORMATION - Please Fill Out CompletelynorniellarNoch keine Bewertungen
- Adult Intake-1Dokument13 SeitenAdult Intake-1Kimberly StanfordNoch keine Bewertungen
- Loh 2012 PDFDokument7 SeitenLoh 2012 PDFJulie Lyles CarrNoch keine Bewertungen
- Akeela House Intake Packet RDokument11 SeitenAkeela House Intake Packet RDamonNoch keine Bewertungen
- Application For Volunteer: Program of InterestDokument2 SeitenApplication For Volunteer: Program of InterestSahar HakimiNoch keine Bewertungen
- New Patient Information-2021Dokument6 SeitenNew Patient Information-2021Anime300Noch keine Bewertungen
- Patient FormsDokument4 SeitenPatient Formsapi-203989638Noch keine Bewertungen
- New Patient FormDokument7 SeitenNew Patient Formhamzahali039Noch keine Bewertungen
- Students With Mental Health Related DisabilitiesDokument11 SeitenStudents With Mental Health Related DisabilitiesMaisie KamalNoch keine Bewertungen
- Advocare Consent Disclosure Authorization PDFDokument2 SeitenAdvocare Consent Disclosure Authorization PDFAsnaifa Bint MamintalNoch keine Bewertungen
- Rachel Mccrickard HandoutDokument4 SeitenRachel Mccrickard Handoutapi-681819056Noch keine Bewertungen
- Sample Annex B - CPM Aug 2022Dokument3 SeitenSample Annex B - CPM Aug 2022Enoel MarkusNoch keine Bewertungen
- Delta Dental 4Dokument3 SeitenDelta Dental 4Yong WeiNoch keine Bewertungen
- Acpe Cpe Spiritual CareDokument2 SeitenAcpe Cpe Spiritual CarematukualfredNoch keine Bewertungen
- Updated VHC NP FormsDokument4 SeitenUpdated VHC NP FormsKipp GillianNoch keine Bewertungen
- Annexure-I Nomination/Registration Form - Applicants of Indian NationalityDokument8 SeitenAnnexure-I Nomination/Registration Form - Applicants of Indian NationalityRohitNoch keine Bewertungen
- Contact With Offender Declaration: ConfidentialDokument4 SeitenContact With Offender Declaration: ConfidentialJohn OhNoch keine Bewertungen
- Hospital VolunteerDokument6 SeitenHospital Volunteermikeross08Noch keine Bewertungen
- New ClientDokument6 SeitenNew Clientapi-312970853Noch keine Bewertungen
- Patient Complaint FormDokument8 SeitenPatient Complaint FormMirza Moazzam BaigNoch keine Bewertungen
- FORM Health HistoryDokument2 SeitenFORM Health HistoryxxxhbkxxxNoch keine Bewertungen
- Doctor Statement Ssa 787Dokument3 SeitenDoctor Statement Ssa 787Richard GuthNoch keine Bewertungen
- New Patient Forms 2018Dokument8 SeitenNew Patient Forms 2018Rexy LasutNoch keine Bewertungen
- Patient Care Coordinator ResumeDokument6 SeitenPatient Care Coordinator Resumeafmsisbmqgpdof100% (1)
- Adult NP Ppwrork KCPGDokument16 SeitenAdult NP Ppwrork KCPGMary GreerNoch keine Bewertungen
- Access Health Enrollment FormsDokument5 SeitenAccess Health Enrollment FormsadeleaNoch keine Bewertungen
- How To Request Your Covid - 19 Lab Report: Complete The Consent To Disclose Phi FormDokument3 SeitenHow To Request Your Covid - 19 Lab Report: Complete The Consent To Disclose Phi FormAnithasree SrinivasanNoch keine Bewertungen
- Application For Admission: General InformationDokument3 SeitenApplication For Admission: General InformationEmily HoeNoch keine Bewertungen
- Secondary Application Form Fall 2013 Entering Class: Mahmood MadihaDokument2 SeitenSecondary Application Form Fall 2013 Entering Class: Mahmood MadihaSumaya MahmoodNoch keine Bewertungen
- Patient Profile FormDokument2 SeitenPatient Profile Formabigaelpanganiban2000Noch keine Bewertungen
- Immmunization FormDokument1 SeiteImmmunization Formnarutokun0Noch keine Bewertungen
- APPLICATIONDokument4 SeitenAPPLICATIONmonalisa molinaNoch keine Bewertungen
- Pediatric New Patient FormDokument13 SeitenPediatric New Patient FormMr. Alma Myers, LAcNoch keine Bewertungen
- 2015 English RegistrationDokument5 Seiten2015 English RegistrationsleaderhNoch keine Bewertungen
- Adult Client Intake Forms2Dokument7 SeitenAdult Client Intake Forms2api-310813184Noch keine Bewertungen
- Griffin Observership ApplicationDokument7 SeitenGriffin Observership Applicationসোমনাথ মহাপাত্রNoch keine Bewertungen
- Legacy Holistic Health Enrollment AgreementDokument14 SeitenLegacy Holistic Health Enrollment AgreementjenniferNoch keine Bewertungen
- How To Become A Mercy General Hospital VolunteerDokument6 SeitenHow To Become A Mercy General Hospital VolunteerShabnam AlizadaNoch keine Bewertungen
- Sample Consent FormDokument4 SeitenSample Consent FormNoe ZalamedaNoch keine Bewertungen
- Salvere Quarterly-Issue 1 Vol 2Dokument3 SeitenSalvere Quarterly-Issue 1 Vol 2Howaida LibyaNoch keine Bewertungen
- Salvere Quarterly-Issue 2 Vol 2Dokument3 SeitenSalvere Quarterly-Issue 2 Vol 2Howaida LibyaNoch keine Bewertungen
- Salvere Quarterly-Issue 1 Vol 2Dokument3 SeitenSalvere Quarterly-Issue 1 Vol 2Howaida LibyaNoch keine Bewertungen
- Superbowl 2014Dokument1 SeiteSuperbowl 2014Howaida LibyaNoch keine Bewertungen
- Super Bowl 2014 at Tripoli'sDokument1 SeiteSuper Bowl 2014 at Tripoli'sHowaida LibyaNoch keine Bewertungen
- Super Bowl 2014 at Tripoli'sDokument1 SeiteSuper Bowl 2014 at Tripoli'sHowaida LibyaNoch keine Bewertungen
- Salvere Quarterly-Issue 3 Vol 1Dokument4 SeitenSalvere Quarterly-Issue 3 Vol 1Howaida LibyaNoch keine Bewertungen
- Super Bowl 2014 at Tripoli'sDokument1 SeiteSuper Bowl 2014 at Tripoli'sHowaida LibyaNoch keine Bewertungen
- Salvere Quarterly-Issue 4 Vol 1Dokument3 SeitenSalvere Quarterly-Issue 4 Vol 1Howaida LibyaNoch keine Bewertungen
- Salvere Quarterly-Issue 2 Vol 1Dokument4 SeitenSalvere Quarterly-Issue 2 Vol 1Howaida LibyaNoch keine Bewertungen
- Salvere Quarterly-Issue 1 Vol 1Dokument2 SeitenSalvere Quarterly-Issue 1 Vol 1Howaida LibyaNoch keine Bewertungen
- Salvere Prenursing Public Health ProgramDokument1 SeiteSalvere Prenursing Public Health ProgramHowaida LibyaNoch keine Bewertungen
- Perspective On Teaching and LearningDokument67 SeitenPerspective On Teaching and LearningJoybelle HarayoNoch keine Bewertungen
- Fusion Center Study Finds 79% of Recent Mass Shootings Attributable To History of Mental Illness - Public IntelligenceDokument11 SeitenFusion Center Study Finds 79% of Recent Mass Shootings Attributable To History of Mental Illness - Public IntelligenceTy UsikNoch keine Bewertungen
- Apps For Paediatric Dosing - An Evaluation - Vonbach PriskaDokument1 SeiteApps For Paediatric Dosing - An Evaluation - Vonbach PriskaSara KreboldNoch keine Bewertungen
- Definition of GriefDokument16 SeitenDefinition of GriefNaveen Eldose100% (1)
- Ectopic PregnancyDokument4 SeitenEctopic PregnancySyahriana AnaNoch keine Bewertungen
- Guidelines For DNR Policies in Nursing FacilitiesDokument2 SeitenGuidelines For DNR Policies in Nursing Facilitiesmichelle marquezNoch keine Bewertungen
- Career Map AssignmentDokument9 SeitenCareer Map Assignmentapi-301456362Noch keine Bewertungen
- Nursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718Dokument14 SeitenNursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718jelaNoch keine Bewertungen
- Community Pantry Guidelines - 23apr21Dokument2 SeitenCommunity Pantry Guidelines - 23apr21Maris Angelica AyuyaoNoch keine Bewertungen
- Case Presentation OralcavityDokument33 SeitenCase Presentation Oralcavityapi-250609678Noch keine Bewertungen
- Counterfeit DrugsDokument2 SeitenCounterfeit DrugsfreeBlidaman0967% (3)
- Test Taking TipsDokument59 SeitenTest Taking TipschelljynxieNoch keine Bewertungen
- High Frequency Oscillatory Ventilation (HFOV) تغريدDokument16 SeitenHigh Frequency Oscillatory Ventilation (HFOV) تغريدtaghreednurseNoch keine Bewertungen
- Growing American Youth CMP FINALDokument43 SeitenGrowing American Youth CMP FINALLaur MarchapNoch keine Bewertungen
- Unit 4 Maternal ConceptsDokument8 SeitenUnit 4 Maternal ConceptsEunice TrinidadNoch keine Bewertungen
- Acceptance LetterDokument40 SeitenAcceptance LetterDonald IbonaNoch keine Bewertungen
- 8 Effect of Exercises in The Management of PDFDokument254 Seiten8 Effect of Exercises in The Management of PDFAmalia RiaNoch keine Bewertungen
- Ballad Scarce Resource Allocation Patient Notification LetterDokument2 SeitenBallad Scarce Resource Allocation Patient Notification LetterJosh Smith100% (1)
- Psychologist Cover Letter ExampleDokument4 SeitenPsychologist Cover Letter Exampleafjzcgeoylbkku100% (2)
- 2014 Resume - Adam SavineDokument1 Seite2014 Resume - Adam SavineAdamSavineNoch keine Bewertungen
- Review Combat Against COVID-19 Complications - Traditional Plant Lantana CamaraDokument5 SeitenReview Combat Against COVID-19 Complications - Traditional Plant Lantana CamaraInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Title of The ResearchDokument5 SeitenTitle of The ResearchNAMAN PARMARNoch keine Bewertungen
- Nurs FPX 4030 Assessment 3 Pico T Questions and An Evidence Based ApproachDokument6 SeitenNurs FPX 4030 Assessment 3 Pico T Questions and An Evidence Based Approachzadem5266Noch keine Bewertungen
- Job Safety Analysis Lifting Cooling TowerDokument4 SeitenJob Safety Analysis Lifting Cooling TowerSeppy FajrianiNoch keine Bewertungen