Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Adult Basic Life Support CPRDokument30 SeitenAdult Basic Life Support CPRRaiz100% (1)
- BLS With MCQDokument37 SeitenBLS With MCQKIMS quality100% (1)
- TAVR Low RiskDokument5 SeitenTAVR Low RiskTom BiusoNoch keine Bewertungen
- Difficult Airway Trolley DASDokument13 SeitenDifficult Airway Trolley DASracut_khansatra50% (2)
- Interventional Nephrology: From Episodic To Coordinated Vascular Access CareDokument8 SeitenInterventional Nephrology: From Episodic To Coordinated Vascular Access Caredal81_aksNoch keine Bewertungen
- Trays That Have Been TaggedDokument6 SeitenTrays That Have Been TaggedJohnny JohnsonNoch keine Bewertungen
- Audit FinalisedDokument346 SeitenAudit FinalisednatheNoch keine Bewertungen
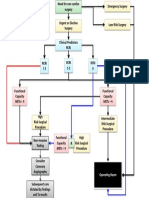
- Cardiac Risk Assessemnt FlowchartDokument1 SeiteCardiac Risk Assessemnt FlowchartjamesomooreNoch keine Bewertungen
- Pha-Bls 2H2019Dokument3 SeitenPha-Bls 2H2019Abram BunoanNoch keine Bewertungen
- Prosedur SirkumsisiDokument20 SeitenProsedur SirkumsisiDamar Nirwan Alby100% (1)
- Ascento Dental Line Catalog Implanturi Alpha Dent GermaniaDokument82 SeitenAscento Dental Line Catalog Implanturi Alpha Dent GermaniaGabriela IconaruNoch keine Bewertungen
- TGS KKPMT Reproduksi WanitaDokument7 SeitenTGS KKPMT Reproduksi WanitaUswatun HasanahNoch keine Bewertungen
- Final Price List New-Suture (CT) - Juni - 2018Dokument47 SeitenFinal Price List New-Suture (CT) - Juni - 2018dian indrayantiNoch keine Bewertungen
- BLS Skills Checklist 2022Dokument4 SeitenBLS Skills Checklist 2022Maric MorganNoch keine Bewertungen
- AngioplastyDokument10 SeitenAngioplastyВлада ХоружийNoch keine Bewertungen
- Data Travelling Pasien HDDokument2 SeitenData Travelling Pasien HDabuyusuf-abuNoch keine Bewertungen
- Introduction To Cosmetic SurgeryDokument2 SeitenIntroduction To Cosmetic SurgeryDeepak GhimireNoch keine Bewertungen
- Cghs RatesDokument111 SeitenCghs RatesHarshvardhan BhardwazNoch keine Bewertungen
- Surgicals RFQ Fy 2024-25Dokument225 SeitenSurgicals RFQ Fy 2024-25Keshav KumarNoch keine Bewertungen
- 7RL Catalogue - Updated Jan 2022Dokument15 Seiten7RL Catalogue - Updated Jan 2022Taiwo FaleyeNoch keine Bewertungen
- Kode ICD 10 Dan ICD 9 Urologi: GinjalDokument1 SeiteKode ICD 10 Dan ICD 9 Urologi: GinjalAkmal FawziNoch keine Bewertungen
- PALES Prog WebDokument15 SeitenPALES Prog WebBGHMC SURGERYNoch keine Bewertungen
- La Moderna Psicocirugía: Un Nuevo Enfoque de La Neurocirugía en La Enfermedad PsiquiátricaDokument11 SeitenLa Moderna Psicocirugía: Un Nuevo Enfoque de La Neurocirugía en La Enfermedad PsiquiátricaLaura De BrigardNoch keine Bewertungen
- MJPJAY Procedures 996Dokument58 SeitenMJPJAY Procedures 996bhushan adhariNoch keine Bewertungen
- Pasien SC Bulan Januari 2019: Tanggal MasukDokument25 SeitenPasien SC Bulan Januari 2019: Tanggal MasukMaria AmabiNoch keine Bewertungen
- Surgical Procedure ClassificationDokument2 SeitenSurgical Procedure ClassificationNeoGellinNoch keine Bewertungen
- Guía de Electrodos Externos Mindray BeneheartDokument1 SeiteGuía de Electrodos Externos Mindray BeneheartBio IngenieriaNoch keine Bewertungen
- Hujiolgy Workstation D05Dokument6 SeitenHujiolgy Workstation D05G.330Noch keine Bewertungen
- Inventory 05.05.2021Dokument18 SeitenInventory 05.05.2021كوكتيل شخابيطNoch keine Bewertungen
- High-Flow Nasal Cannula Pada Anak (Literatur Review) : Avalilable OnlineDokument12 SeitenHigh-Flow Nasal Cannula Pada Anak (Literatur Review) : Avalilable Onlinejeinzen14Noch keine Bewertungen