Das könnte Ihnen auch gefallen
- NIH Public Access: Author ManuscriptDokument20 SeitenNIH Public Access: Author ManuscriptSarif CassanovaNoch keine Bewertungen
- BouhnikDokument9 SeitenBouhnikSarif CassanovaNoch keine Bewertungen
- Rekap Anggota DPD Ipai Sulawesi Selatan Dan Barat: Tana TorajaDokument3 SeitenRekap Anggota DPD Ipai Sulawesi Selatan Dan Barat: Tana TorajaSarif CassanovaNoch keine Bewertungen
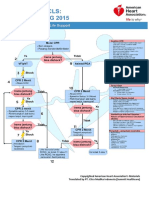
- Algoritma ACLS Bhs IndonesiaDokument6 SeitenAlgoritma ACLS Bhs IndonesiaSarif CassanovaNoch keine Bewertungen
- Management of Foreskin ConditionsDokument26 SeitenManagement of Foreskin ConditionsSarif CassanovaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Case Study 5.6.1 JOHNSON AND JOHNSONDokument2 SeitenCase Study 5.6.1 JOHNSON AND JOHNSONnaman0% (1)
- DPN Icu PDFDokument1 SeiteDPN Icu PDFharoonNoch keine Bewertungen
- Florida Physician Database - Areas Includes Gainesville, Orlando and JacksonvilleDokument20 SeitenFlorida Physician Database - Areas Includes Gainesville, Orlando and JacksonvilleBhuvana RajendranNoch keine Bewertungen
- MLT Student NotesDokument5 SeitenMLT Student NotesClaire GonzalesNoch keine Bewertungen
- Tramadol, Paracetamol, Calmoseptine, B12Dokument5 SeitenTramadol, Paracetamol, Calmoseptine, B12Denise EspinosaNoch keine Bewertungen
- Sekilas Info: CardiomyopathyDokument15 SeitenSekilas Info: CardiomyopathyZukmianty SuaibNoch keine Bewertungen
- Alexandra Mcfall - Annotated BibliographyDokument6 SeitenAlexandra Mcfall - Annotated Bibliographyapi-549246948Noch keine Bewertungen
- JuRnal 6 PDFDokument8 SeitenJuRnal 6 PDFNurhajar AzzahraNoch keine Bewertungen
- DisabilityDokument450 SeitenDisabilityTony Kelbrat100% (1)
- GH 13 600Dokument9 SeitenGH 13 600Gar BettaNoch keine Bewertungen
- Rituximab Tullus Kjeil 2021Dokument9 SeitenRituximab Tullus Kjeil 2021Carmen MunteanNoch keine Bewertungen
- 4th Week Health ModulesDokument13 Seiten4th Week Health ModulesYza VelleNoch keine Bewertungen
- Patel 2013Dokument8 SeitenPatel 2013joantyy 1Noch keine Bewertungen
- 4788 ID Faktor Risiko Lingkungan Kejadian Leptospirosis Di Jawa Tengah Studi Kasus Di Ko PDFDokument8 Seiten4788 ID Faktor Risiko Lingkungan Kejadian Leptospirosis Di Jawa Tengah Studi Kasus Di Ko PDFbintang nurzakiahNoch keine Bewertungen
- CONFUSION TextoDokument15 SeitenCONFUSION TextoBarbara SolangeNoch keine Bewertungen
- Sean Benesh Resume 10-1-23Dokument2 SeitenSean Benesh Resume 10-1-23api-708800698Noch keine Bewertungen
- Respiratory MCQDokument24 SeitenRespiratory MCQfrabziNoch keine Bewertungen
- Pathophysiology of Septic ShockDokument19 SeitenPathophysiology of Septic ShockRoberto López MataNoch keine Bewertungen
- Role of Presepsin in Determining The Incidence of Septic Shock and Mortality in Patients With SepsisDokument8 SeitenRole of Presepsin in Determining The Incidence of Septic Shock and Mortality in Patients With Sepsisfaraz.mirza1Noch keine Bewertungen
- Hospital Payment Systems Based On DiagnosisDokument16 SeitenHospital Payment Systems Based On DiagnosisErma HandayaniNoch keine Bewertungen
- The Prevalence of Severe Malaria in Children Below Five Years of Age at Hoima Regional Referral Hospital, Hoima CityDokument9 SeitenThe Prevalence of Severe Malaria in Children Below Five Years of Age at Hoima Regional Referral Hospital, Hoima CityKIU PUBLICATION AND EXTENSIONNoch keine Bewertungen
- Homeopathy and Placebo - Synonym, Similar or Different?: Frank Zimmermann-Viehoff Karin MeissnerDokument2 SeitenHomeopathy and Placebo - Synonym, Similar or Different?: Frank Zimmermann-Viehoff Karin MeissnerSaim ShahNoch keine Bewertungen
- Community - Based NursingDokument16 SeitenCommunity - Based NursingManu CvNoch keine Bewertungen
- Developmental Endocrine Reproductive Toxicologist in NJ NY Resume Edward FrizellDokument7 SeitenDevelopmental Endocrine Reproductive Toxicologist in NJ NY Resume Edward FrizellEdwardFrizellNoch keine Bewertungen
- Vibrio Cholerae PosterDokument1 SeiteVibrio Cholerae PosterStela MonkNoch keine Bewertungen
- The Icd - 10 DictionaryDokument10 SeitenThe Icd - 10 DictionarySeraphin MulambaNoch keine Bewertungen
- PCOL Notes 001 IntroDokument1 SeitePCOL Notes 001 IntroCansNoch keine Bewertungen
- Or NCP (Risk For Infection)Dokument1 SeiteOr NCP (Risk For Infection)Nikki M. Arapol100% (1)
- Stroke Mimics: Clinical and Radiological Evaluation: Poster No.: Congress: Type: Authors: KeywordsDokument20 SeitenStroke Mimics: Clinical and Radiological Evaluation: Poster No.: Congress: Type: Authors: KeywordsOrlin ZlatarskiNoch keine Bewertungen
- BHW Reference Manual and Playbook - TagalogDokument136 SeitenBHW Reference Manual and Playbook - TagalogCarlen Mae L. YacapinNoch keine Bewertungen