Das könnte Ihnen auch gefallen
- TracheostomyDokument8 SeitenTracheostomySeree Nah TRNoch keine Bewertungen
- Tracheotomy - Emergency Airway ManagementDokument11 SeitenTracheotomy - Emergency Airway ManagementVladNoch keine Bewertungen
- Tracheostomy Training Resources: A Guide To Tracheostomy Management in Critical Care and BeyondDokument70 SeitenTracheostomy Training Resources: A Guide To Tracheostomy Management in Critical Care and BeyondMarwah Alnoor YousufNoch keine Bewertungen
- What You Need To Know About Tracheostomy 2020Dokument10 SeitenWhat You Need To Know About Tracheostomy 2020Agata KaczmarekNoch keine Bewertungen
- TracheostomyDokument4 SeitenTracheostomyNapieh Bulalaque PolisticoNoch keine Bewertungen
- Tracheostomy OverviewDokument9 SeitenTracheostomy Overview8pvz96ktd9Noch keine Bewertungen
- 241 TracheostomyDokument12 Seiten241 Tracheostomyalbert hutagalungNoch keine Bewertungen
- Assignment On TreacheostomyDokument7 SeitenAssignment On Treacheostomysantosh kumarNoch keine Bewertungen
- MedSurg NotesDokument57 SeitenMedSurg NotesCHRISTOFER CORONADONoch keine Bewertungen
- TRACHEOSTOMYDokument2 SeitenTRACHEOSTOMY3C SAVELLA, Glaiza Marie RNoch keine Bewertungen
- Tracheostomy: Continuing Education ActivityDokument9 SeitenTracheostomy: Continuing Education ActivityUlul IsmiNoch keine Bewertungen
- Airway Management: Intensive Care Unit, Prince of Wales Hospital, Chinese University of Hong KongDokument9 SeitenAirway Management: Intensive Care Unit, Prince of Wales Hospital, Chinese University of Hong KongErwinRamadhaniNoch keine Bewertungen
- Endotracheal TubeDokument19 SeitenEndotracheal TubeSarvess Muniandy100% (1)
- Tracheostomy Tube CareDokument12 SeitenTracheostomy Tube CareydtrgnNoch keine Bewertungen
- Clinical Guidelines (Nursing) : Tracheostomy ManagementDokument19 SeitenClinical Guidelines (Nursing) : Tracheostomy ManagementbarbiemeNoch keine Bewertungen
- TracheostomyDokument28 SeitenTracheostomyprivatejarjarbinksNoch keine Bewertungen
- Tracheostomy Care (Done)Dokument53 SeitenTracheostomy Care (Done)martinNoch keine Bewertungen
- Laboratory Unit 3 1Dokument6 SeitenLaboratory Unit 3 1Mushy_ayaNoch keine Bewertungen
- Tracheostomy Tubes Careand CleaningDokument18 SeitenTracheostomy Tubes Careand CleaningMasango ChristopherNoch keine Bewertungen
- Tracheostomy: Presented By: Barte, Hannah Aida D. Balamurugan, RameebhaDokument21 SeitenTracheostomy: Presented By: Barte, Hannah Aida D. Balamurugan, RameebhaThakoon Tts100% (1)
- Tracheostomy: ENT Department DMC & Hospital Ludhiana PunjabDokument46 SeitenTracheostomy: ENT Department DMC & Hospital Ludhiana PunjabVikrant MittalNoch keine Bewertungen
- TracheostomyDokument27 SeitenTracheostomynahidanila439Noch keine Bewertungen
- TracheostomyDokument35 SeitenTracheostomyAbdur Raqib100% (1)
- Assissting IntubationDokument17 SeitenAssissting IntubationTriciaNoch keine Bewertungen
- Guideline of Tracheostomy in Adult CareDokument3 SeitenGuideline of Tracheostomy in Adult CareAlvin NGNoch keine Bewertungen
- 2021 - 2022 Tracheostomy Care ProcedureDokument69 Seiten2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNoch keine Bewertungen
- 2021 - 2022 Tracheostomy Care ProcedureDokument69 Seiten2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNoch keine Bewertungen
- Dona Remedios Trinidad Romualdez Medical Foundation College of Nursing Worksheet On NCM 109 - RLE Concept: Nursing Procedures Related To Oxygenation (Respiratory System)Dokument18 SeitenDona Remedios Trinidad Romualdez Medical Foundation College of Nursing Worksheet On NCM 109 - RLE Concept: Nursing Procedures Related To Oxygenation (Respiratory System)Franz Earl Niño AlbesaNoch keine Bewertungen
- TracheostomyDokument63 SeitenTracheostomyAyesha FayyazNoch keine Bewertungen
- Tracheostomy Operating TechniqueDokument34 SeitenTracheostomy Operating TechniqueIsa BasukiNoch keine Bewertungen
- CricothyroidotomyDokument38 SeitenCricothyroidotomyAlsalman AnamNoch keine Bewertungen
- Rapid Sequence Intubation ReportDokument55 SeitenRapid Sequence Intubation Reportlorkan19100% (1)
- TracheostomyDokument4 SeitenTracheostomySuchismita SethiNoch keine Bewertungen
- Amit Tracheostomy Presentation 12 Aug 2010Dokument59 SeitenAmit Tracheostomy Presentation 12 Aug 2010Amit KochetaNoch keine Bewertungen
- Annrcse01509 0sutureDokument3 SeitenAnnrcse01509 0sutureNichole Audrey SaavedraNoch keine Bewertungen
- Endotracheal Intubation Learning MaterialDokument8 SeitenEndotracheal Intubation Learning MaterialLouie ParillaNoch keine Bewertungen
- Long-Term Complications of Tracheal IntubationDokument24 SeitenLong-Term Complications of Tracheal Intubationandi kurniawanNoch keine Bewertungen
- Ateneo de Zamboanga University: Nursing Skills Output (Nso)Dokument9 SeitenAteneo de Zamboanga University: Nursing Skills Output (Nso)Mitzi BelamideNoch keine Bewertungen
- Tracheostomy in Palliative CaraDokument9 SeitenTracheostomy in Palliative CarameritaNoch keine Bewertungen
- TracheostomyDokument36 SeitenTracheostomyjacnpoyNoch keine Bewertungen
- What Is A Tracheostomy? Why Is A Tracheostomy Performed?Dokument5 SeitenWhat Is A Tracheostomy? Why Is A Tracheostomy Performed?Mara JnelleNoch keine Bewertungen
- The Changing Role For Tracheostomy in Patients Requiring Mechanical VentilationDokument11 SeitenThe Changing Role For Tracheostomy in Patients Requiring Mechanical VentilationGhost11mNoch keine Bewertungen
- Decanulasi TrakeostomiDokument6 SeitenDecanulasi TrakeostomiDhiel Muhammad FarreyraNoch keine Bewertungen
- Issaiah Nicolle L. Cecilia 3 BSN - ADokument6 SeitenIssaiah Nicolle L. Cecilia 3 BSN - AIssaiah Nicolle CeciliaNoch keine Bewertungen
- Tracheostomy Activity: /admendoza2020Dokument2 SeitenTracheostomy Activity: /admendoza2020FranchieNoch keine Bewertungen
- Complications of Endotracheal Intubation and Other Airway Management ProceduresDokument11 SeitenComplications of Endotracheal Intubation and Other Airway Management ProceduresashajangamNoch keine Bewertungen
- Et TubeDokument31 SeitenEt Tubeinno so qtNoch keine Bewertungen
- Physiotherapy in General Surgical ConditionDokument7 SeitenPhysiotherapy in General Surgical Conditionprofpt98100% (8)
- Egyptian Journal of Ear, Nose, Throat and Allied SciencesDokument5 SeitenEgyptian Journal of Ear, Nose, Throat and Allied SciencesLuis De jesus SolanoNoch keine Bewertungen
- Complications of Endotracheal Intubation and Other Airway Management ProceduresDokument11 SeitenComplications of Endotracheal Intubation and Other Airway Management ProceduresSuresh Kumar100% (1)
- Final Content ET Intubation 1Dokument27 SeitenFinal Content ET Intubation 1Debipriya MistryNoch keine Bewertungen
- Howard B. Seim III, DVM, DACVS Colorado State University: WWW - VideovetorgDokument4 SeitenHoward B. Seim III, DVM, DACVS Colorado State University: WWW - VideovetorgIkhsan HidayatNoch keine Bewertungen
- Tracheostomy 191224152833Dokument106 SeitenTracheostomy 191224152833Dimas SevantoNoch keine Bewertungen
- E T IntubationDokument15 SeitenE T Intubationjtalan9Noch keine Bewertungen
- Handout TracheostomyDokument1 SeiteHandout TracheostomyDhAiRyA ArOrANoch keine Bewertungen
- Issaiah Nicolle L. Cecilia 3 BSN - ADokument14 SeitenIssaiah Nicolle L. Cecilia 3 BSN - AIssaiah Nicolle CeciliaNoch keine Bewertungen
- Tracheostomy Suctioning and HumidificationDokument5 SeitenTracheostomy Suctioning and HumidificationLucila LugoNoch keine Bewertungen
- Postlaryngectomy voice rehabilitation with voice prosthesesVon EverandPostlaryngectomy voice rehabilitation with voice prosthesesNoch keine Bewertungen
- Carbrain c168 User Manual 2Dokument25 SeitenCarbrain c168 User Manual 2mindreader19Noch keine Bewertungen
- Assessment of Vital Signs: Marie Bártová, BSNDokument16 SeitenAssessment of Vital Signs: Marie Bártová, BSNmindreader19Noch keine Bewertungen
- Nursing Interventions in Anxiety: General Principles Nursing ConsiderationsDokument7 SeitenNursing Interventions in Anxiety: General Principles Nursing Considerationsmindreader19Noch keine Bewertungen
- 32Dokument32 Seiten32mindreader19Noch keine Bewertungen
- Table 2a Diabetes Mellitus: Level of Awareness Among Residents of Brgy. 9, Tigbauan, Iloilo When Taken As A WholeDokument2 SeitenTable 2a Diabetes Mellitus: Level of Awareness Among Residents of Brgy. 9, Tigbauan, Iloilo When Taken As A Wholemindreader19Noch keine Bewertungen
- Normal ValuesDokument6 SeitenNormal Valuesmindreader19Noch keine Bewertungen
- The Story of Labaw DonggonDokument8 SeitenThe Story of Labaw Donggonmindreader19Noch keine Bewertungen
- DirectingDokument11 SeitenDirectingmindreader19Noch keine Bewertungen
- The Story of Labaw Donggon FINALDokument9 SeitenThe Story of Labaw Donggon FINALmindreader19100% (1)
- The Heart of Managerial ProcessDokument72 SeitenThe Heart of Managerial Processmindreader19Noch keine Bewertungen
- DirectingDokument11 SeitenDirectingmindreader19Noch keine Bewertungen
- Area A1Dokument1 SeiteArea A1mindreader19Noch keine Bewertungen
- DTC P0171 System Too Lean (Fuel Trim) : Circuit DescriptionDokument4 SeitenDTC P0171 System Too Lean (Fuel Trim) : Circuit Descriptionmindreader19Noch keine Bewertungen
- No. of Respondents Awareness Preventive Practices Age Gender QuestionsDokument1 SeiteNo. of Respondents Awareness Preventive Practices Age Gender Questionsmindreader19Noch keine Bewertungen
- Annotated BibliographyDokument3 SeitenAnnotated Bibliographyapi-462495619Noch keine Bewertungen
- National Drug Policy 1995Dokument13 SeitenNational Drug Policy 1995Madhu Sudhan PandeyaNoch keine Bewertungen
- The 10 Most (And Least) Prestigious Jobs in AmericaDokument12 SeitenThe 10 Most (And Least) Prestigious Jobs in AmericaParlindungan PardedeNoch keine Bewertungen
- University of Illinois College of Medicine at Rockford Match List - Class of 2019Dokument2 SeitenUniversity of Illinois College of Medicine at Rockford Match List - Class of 2019Jeff KolkeyNoch keine Bewertungen
- Preface: A Collection of Previous Year Question Papers of NEET and AIIMS ExaminationsDokument9 SeitenPreface: A Collection of Previous Year Question Papers of NEET and AIIMS ExaminationsAsmitNoch keine Bewertungen
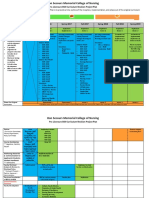
- BSN Curriculum Revision Project Plan 2Dokument2 SeitenBSN Curriculum Revision Project Plan 2api-372924050Noch keine Bewertungen
- Nursing Standards of PracticeDokument24 SeitenNursing Standards of Practiceapi-238698438Noch keine Bewertungen
- Interprofessional Collaboration: Running HeadDokument6 SeitenInterprofessional Collaboration: Running HeadJoseph KaruguNoch keine Bewertungen
- 0 - Reflection MCNDokument1 Seite0 - Reflection MCNVanessa Mae IlaganNoch keine Bewertungen
- RA 7875 Amended by RA 11223 Universal Health Care ActDokument21 SeitenRA 7875 Amended by RA 11223 Universal Health Care ActChristopher AdvinculaNoch keine Bewertungen
- Statement of PurposeDokument2 SeitenStatement of PurposeTara GonzalesNoch keine Bewertungen
- PiVOT IIPPE 22 Regulatory ScienceDokument7 SeitenPiVOT IIPPE 22 Regulatory SciencesherlockNoch keine Bewertungen
- Penilaian Preceptorship (Mini-Cex, Dops, Longcase, Soca) 2020Dokument49 SeitenPenilaian Preceptorship (Mini-Cex, Dops, Longcase, Soca) 2020Dian tri febrianaNoch keine Bewertungen
- CMAM Training PPT 2018 - 0Dokument57 SeitenCMAM Training PPT 2018 - 0cabdinuux32Noch keine Bewertungen
- DetailingDokument5 SeitenDetailingNoor MuhammadNoch keine Bewertungen
- Sources of StrengthDokument26 SeitenSources of StrengthMYRA R. SABEROLANoch keine Bewertungen
- MGN815: Business Models: Ajay ChandelDokument21 SeitenMGN815: Business Models: Ajay ChandelSam RehmanNoch keine Bewertungen
- Understanding Health Insurance Literacy A Literature ReviewDokument7 SeitenUnderstanding Health Insurance Literacy A Literature ReviewafduadazaNoch keine Bewertungen
- Assessing Pulse Oximetry (Performance Checklist) : Iloilo Doctors' College College of NursingDokument1 SeiteAssessing Pulse Oximetry (Performance Checklist) : Iloilo Doctors' College College of NursingJemy Tamaño MorongNoch keine Bewertungen
- BALNEOTHERAPY IN PATIENTS WITH PARkINSON'S DISEASEDokument6 SeitenBALNEOTHERAPY IN PATIENTS WITH PARkINSON'S DISEASEThermalBathsforActivNoch keine Bewertungen
- MHI2017 Assignment 4Dokument19 SeitenMHI2017 Assignment 4Dr. Aby Mathews MaluvelilNoch keine Bewertungen
- Hubungan Mean Arterial Pressure Dengan Kejadian MualDokument3 SeitenHubungan Mean Arterial Pressure Dengan Kejadian MualMuhardi Deviko PutraNoch keine Bewertungen
- Counselling in A Digital WorldDokument2 SeitenCounselling in A Digital WorldIhin Nur FarihinNoch keine Bewertungen
- Paracetamol IV AmpuleDokument3 SeitenParacetamol IV AmpuleEli Thy IgopNoch keine Bewertungen
- LMRASSIGNMENTDokument2 SeitenLMRASSIGNMENTjaoNoch keine Bewertungen
- Paper II Part: General SubjectDokument2 SeitenPaper II Part: General SubjectAshutosh MurawNoch keine Bewertungen
- Veteran Help-Seeking Behaviour For Mental HealthDokument6 SeitenVeteran Help-Seeking Behaviour For Mental HealthDaniel KoffmanNoch keine Bewertungen
- Cme - InvitationDokument3 SeitenCme - InvitationANATOMY GKMCNoch keine Bewertungen
- Anatomy and Physiology of Female For Cesarean SectionDokument8 SeitenAnatomy and Physiology of Female For Cesarean SectionGrace Mellaine100% (1)
- Test AxaDokument2 SeitenTest AxaElmedina Berin HalilovićNoch keine Bewertungen