Das könnte Ihnen auch gefallen
- Histology and Histopathology of the Eye and Its AdnexaVon EverandHistology and Histopathology of the Eye and Its AdnexaNoch keine Bewertungen
- Microbiology 19 PDFDokument6 SeitenMicrobiology 19 PDFLyka Villagracia AsiloNoch keine Bewertungen
- PATHOPHYSIOLOGY of PNEUMONIADokument1 SeitePATHOPHYSIOLOGY of PNEUMONIAElva Borlado BilocuraNoch keine Bewertungen
- Pearls Nov Dec 2010Dokument3 SeitenPearls Nov Dec 2010Nhật LongNoch keine Bewertungen
- February 2016 Ophthalmic Pearls PDFDokument3 SeitenFebruary 2016 Ophthalmic Pearls PDFIndah IndrianiNoch keine Bewertungen
- Conjunctivitis 161031150615Dokument282 SeitenConjunctivitis 161031150615huzefa100% (1)
- L7.3-SURG-Colon, Rectum, Anus, and The Appendix (Mar2022)Dokument3 SeitenL7.3-SURG-Colon, Rectum, Anus, and The Appendix (Mar2022)Erald PaderangaNoch keine Bewertungen
- Periodontal Pathogenesis SalinanDokument66 SeitenPeriodontal Pathogenesis SalinanEka RahayuNoch keine Bewertungen
- Glossary of Periodontal Terms PDFDokument56 SeitenGlossary of Periodontal Terms PDFCarlos Gilberto Guillaumin EsparzaNoch keine Bewertungen
- Bacteria-Borne Diseases Handout 2022Dokument3 SeitenBacteria-Borne Diseases Handout 2022Anna CrisNoch keine Bewertungen
- Eyelids and Lacrimal ApparatusDokument6 SeitenEyelids and Lacrimal Apparatussarguss14Noch keine Bewertungen
- Opthal Book Piyush SirDokument210 SeitenOpthal Book Piyush Sirselmon468Noch keine Bewertungen
- Patologi Sistem Reproduksi WanitaDokument5 SeitenPatologi Sistem Reproduksi WanitaAnjayNoch keine Bewertungen
- Case Report: A Large Extragnathic Keratocystic Odontogenic TumourDokument8 SeitenCase Report: A Large Extragnathic Keratocystic Odontogenic TumourShinta Dewi NNoch keine Bewertungen
- Surgery 421Dokument218 SeitenSurgery 421AshNoch keine Bewertungen
- 01 Introduction To Corneal DiseaseDokument10 Seiten01 Introduction To Corneal DiseaseTrang Nguyễn ThuỳNoch keine Bewertungen
- M100 ActivityDokument5 SeitenM100 ActivityAira Galinato CabrasNoch keine Bewertungen
- Pa MataDokument115 SeitenPa MataIchsan WidjanarkoNoch keine Bewertungen
- ANCYLOSTOMA DUODENALE Old World HookwormDokument2 SeitenANCYLOSTOMA DUODENALE Old World HookwormScarlet AdolfoNoch keine Bewertungen
- 02 Anatomy and Histology PLE 2019 RatioDokument69 Seiten02 Anatomy and Histology PLE 2019 RatioPatricia VillegasNoch keine Bewertungen
- Konjungtivitis GonoreDokument2 SeitenKonjungtivitis Gonorefk unswagatiNoch keine Bewertungen
- Intestinal ObstructionDokument35 SeitenIntestinal Obstructionwht89100% (1)
- Actinomycosis and NOMADokument10 SeitenActinomycosis and NOMASOUMYA A DR, DEPT.OF DENTAL SCIENCES,SRIHERNoch keine Bewertungen
- Section 3-7 Slides + CommentsDokument9 SeitenSection 3-7 Slides + CommentsNkgivgNoch keine Bewertungen
- Ophthalmology - Diseases of CorneaDokument18 SeitenOphthalmology - Diseases of CorneajbtcmdtjjvNoch keine Bewertungen
- Mata Merah 2Dokument26 SeitenMata Merah 2Miftahuljnh01Noch keine Bewertungen
- High Fever Stiff Neck Severe HeadacheDokument3 SeitenHigh Fever Stiff Neck Severe HeadacheDiana Jane LauretaNoch keine Bewertungen
- PATHOPHYSIOLOGY of NeurocysticercosisDokument6 SeitenPATHOPHYSIOLOGY of Neurocysticercosisteddydeclines14100% (3)
- Affections of CorneaDokument9 SeitenAffections of CorneaKirti JamwalNoch keine Bewertungen
- Dilemma in Management of Cervico-Facial Cystic HygromaDokument25 SeitenDilemma in Management of Cervico-Facial Cystic HygromaDR NASIMNoch keine Bewertungen
- Disseminated PorokeratosisDokument3 SeitenDisseminated PorokeratosisMostafaAhmedNoch keine Bewertungen
- CORNEADokument38 SeitenCORNEASamirNoch keine Bewertungen
- B14PathologyL1 - Diseases of The Vulva, Vaginal, and CervixDokument14 SeitenB14PathologyL1 - Diseases of The Vulva, Vaginal, and CervixBarda GulanNoch keine Bewertungen
- PPTXDokument47 SeitenPPTXJu JuNoch keine Bewertungen
- Allergic and Immunologic Eye DiseaseDokument17 SeitenAllergic and Immunologic Eye DiseaseTatiana RecinosNoch keine Bewertungen
- GYNE 4.02 - Lower and Upper Genital InfectionDokument12 SeitenGYNE 4.02 - Lower and Upper Genital InfectionGray Snell100% (1)
- Introduction of Marine Parasite in Malaysia: Prepared by Mohd Adib Fadhil Mohd Arif Bin Mohammad Nor Mohd Hafidz AidzatDokument28 SeitenIntroduction of Marine Parasite in Malaysia: Prepared by Mohd Adib Fadhil Mohd Arif Bin Mohammad Nor Mohd Hafidz AidzatmadibfadhilNoch keine Bewertungen
- Periodontal PocketDokument34 SeitenPeriodontal PocketPrathik RaiNoch keine Bewertungen
- GYNE 2.01a Lower Genital Tract Infections PDFDokument12 SeitenGYNE 2.01a Lower Genital Tract Infections PDFMiguel Domingo100% (1)
- Lab - Benign and MalignantDokument9 SeitenLab - Benign and Malignantkimkaigel6Noch keine Bewertungen
- Contagious Diseases in PHDokument10 SeitenContagious Diseases in PHJEnLipataNoch keine Bewertungen
- Intestinalobstruction: R.Nandinii Group K1Dokument35 SeitenIntestinalobstruction: R.Nandinii Group K1Radityo Budi LeksonoNoch keine Bewertungen
- Oral Pathology: Dr. Tasnim Hamdan Graduated From University of ValenciaDokument160 SeitenOral Pathology: Dr. Tasnim Hamdan Graduated From University of ValenciaMariam Abd ElhadiNoch keine Bewertungen
- Seminar On Septic ArthritisDokument44 SeitenSeminar On Septic ArthritisÇağrıNoch keine Bewertungen
- Cornea: Dr. Izar Aziz, DR., SPM (K)Dokument30 SeitenCornea: Dr. Izar Aziz, DR., SPM (K)Anonymous HgX3mN1oNoch keine Bewertungen
- Schistosoma Haematobium: Dr. Shatarupa ChakrabortyDokument30 SeitenSchistosoma Haematobium: Dr. Shatarupa ChakrabortyRaihanur KiranNoch keine Bewertungen
- Perio Micro 2nd YrDokument33 SeitenPerio Micro 2nd Yrsoni bistaNoch keine Bewertungen
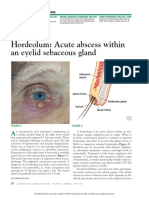
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDokument3 SeitenHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNoch keine Bewertungen
- 1 Cell As A Unit of Health and DiseaseDokument4 Seiten1 Cell As A Unit of Health and DiseaseDonna DominnoNoch keine Bewertungen
- Micro-Para Practical Exam ReviewerDokument8 SeitenMicro-Para Practical Exam ReviewerRA TranceNoch keine Bewertungen
- Intussusception TransDokument4 SeitenIntussusception TransJames Maravillas100% (1)
- Lower Genital Tract InfectionsDokument12 SeitenLower Genital Tract InfectionsIsabel CastilloNoch keine Bewertungen
- Caseous LymphadenitisDokument14 SeitenCaseous LymphadenitismedinamargaretkellyNoch keine Bewertungen
- Insect BitesDokument26 SeitenInsect BiteszeniafadilaNoch keine Bewertungen
- Epithelial and Non-Epithelial Tumor of JawsDokument66 SeitenEpithelial and Non-Epithelial Tumor of JawsDinesh YadavNoch keine Bewertungen
- SubcutaneousDokument2 SeitenSubcutaneousMary ChristelleNoch keine Bewertungen
- Kuliah KarditisDokument50 SeitenKuliah KarditisMuzayyanatulhayat ARNoch keine Bewertungen
- Communicable DiseasesDokument8 SeitenCommunicable DiseasesJamie John EsplanadaNoch keine Bewertungen
- L10.3-OPHTHA-Uvea (Sept3022)Dokument5 SeitenL10.3-OPHTHA-Uvea (Sept3022)Erald PaderangaNoch keine Bewertungen
- Epidural and Spinal AnesthesiaDokument86 SeitenEpidural and Spinal Anesthesiasarguss1471% (7)
- Axial Arthritis: Degenerative Annular DiseaseDokument18 SeitenAxial Arthritis: Degenerative Annular Diseasesarguss14100% (1)
- Cyanotic Congenital Heart Diseases, Etc.Dokument12 SeitenCyanotic Congenital Heart Diseases, Etc.sarguss14100% (2)
- Small BowelDokument4 SeitenSmall Bowelsarguss14100% (1)
- Inhalational Anesthetics: Patigas, Requinta, ResuelloDokument88 SeitenInhalational Anesthetics: Patigas, Requinta, Resuellosarguss140% (1)
- Stage 1: Dorsal Induction: Pediatric NeuroradiologyDokument8 SeitenStage 1: Dorsal Induction: Pediatric Neuroradiologysarguss14100% (1)
- NeuroradiologyDokument11 SeitenNeuroradiologysarguss14100% (2)
- Cardiac ImagingDokument7 SeitenCardiac Imagingsarguss14Noch keine Bewertungen
- Gallbladder, Liver, Pancreas and SpleenDokument19 SeitenGallbladder, Liver, Pancreas and Spleensarguss14100% (3)
- Kidney, Ureter, BladderDokument12 SeitenKidney, Ureter, Bladdersarguss14100% (1)
- Developmental AssessmentDokument3 SeitenDevelopmental Assessmentsarguss14Noch keine Bewertungen
- Pediatric GI RadiologyDokument6 SeitenPediatric GI Radiologysarguss14Noch keine Bewertungen
- From Doc Bandong's Own Words:: Shar 1 of 20Dokument20 SeitenFrom Doc Bandong's Own Words:: Shar 1 of 20sarguss14100% (1)
- Congenital Cystic Adenomatoid Malformation (CCAM)Dokument7 SeitenCongenital Cystic Adenomatoid Malformation (CCAM)sarguss14Noch keine Bewertungen
- Bone TumorsDokument15 SeitenBone Tumorssarguss1450% (2)
- Substance AbuseDokument4 SeitenSubstance Abusesarguss14Noch keine Bewertungen
- Genitourinary SystemDokument8 SeitenGenitourinary Systemsarguss14100% (1)
- Pleura and MediastinumDokument16 SeitenPleura and Mediastinumsarguss14100% (1)
- NeuroradiologyDokument25 SeitenNeuroradiologysarguss14100% (2)
- Mental Retardation and Learning DisordersDokument4 SeitenMental Retardation and Learning Disorderssarguss14100% (1)
- Dissociative and Eating DisordersDokument6 SeitenDissociative and Eating Disorderssarguss14Noch keine Bewertungen
- Introduction To RadiologyDokument3 SeitenIntroduction To Radiologysarguss14Noch keine Bewertungen
- The Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract InfectionsDokument4 SeitenThe Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract Infectionssarguss14Noch keine Bewertungen
- Child Abuse and NeglectDokument3 SeitenChild Abuse and Neglectsarguss14Noch keine Bewertungen
- DepressionDokument3 SeitenDepressionsarguss14Noch keine Bewertungen
- Bipolar DisordersDokument8 SeitenBipolar Disorderssarguss14100% (2)
- Pediatric Endocrinology Part 2: Pediatrics 2Dokument8 SeitenPediatric Endocrinology Part 2: Pediatrics 2sarguss14Noch keine Bewertungen
- Respiratory Distress of The NewbornDokument3 SeitenRespiratory Distress of The Newbornsarguss14100% (1)
- A Dental Home For PWAs 131027Dokument74 SeitenA Dental Home For PWAs 131027Autism Society PhilippinesNoch keine Bewertungen
- Antimalarials - Are They Effective and Safe in Rheumatic DiseasesDokument10 SeitenAntimalarials - Are They Effective and Safe in Rheumatic DiseasesYahya RizkiNoch keine Bewertungen
- Operative Hand InstrumentsDokument22 SeitenOperative Hand InstrumentsSharad Banker50% (2)
- Clinical Pharmacy Answer Key-GREEN PACOP PDFDokument23 SeitenClinical Pharmacy Answer Key-GREEN PACOP PDFOdy100% (3)
- LGU Validation ToolDokument22 SeitenLGU Validation ToolKirsten Calvo100% (3)
- The Miraculous Healing Properties of Oak BarkDokument4 SeitenThe Miraculous Healing Properties of Oak BarkabbajieNoch keine Bewertungen
- Sri Lanka NMRA GazetteDokument9 SeitenSri Lanka NMRA GazetteSanjeev JayaratnaNoch keine Bewertungen
- Review of Electron Beam Therapy PhysicsDokument36 SeitenReview of Electron Beam Therapy PhysicsMaría José Sánchez LovellNoch keine Bewertungen
- AnthropometricDokument11 SeitenAnthropometricdrrebaNoch keine Bewertungen
- TRIKATUDokument5 SeitenTRIKATUAngshuman DuttaNoch keine Bewertungen
- Endorsement Template SURGERYDokument2 SeitenEndorsement Template SURGERYElizalde HusbandNoch keine Bewertungen
- Dermocalm LotionDokument5 SeitenDermocalm LotionSai KrishnaNoch keine Bewertungen
- CELECOXIBDokument1 SeiteCELECOXIBRicky Ramos Jr.Noch keine Bewertungen
- Regulatory Compliance Pharmacy Manager in Tampa FL Resume John HawesDokument2 SeitenRegulatory Compliance Pharmacy Manager in Tampa FL Resume John HawesJohnHawesNoch keine Bewertungen
- Template For Care Plan AssignmentDokument8 SeitenTemplate For Care Plan AssignmentAnn OgoloNoch keine Bewertungen
- Morning Report: Supervisor: Dr. Rusdhy A.H., SP - OG Medical StudentsDokument8 SeitenMorning Report: Supervisor: Dr. Rusdhy A.H., SP - OG Medical StudentsEra MoetzNoch keine Bewertungen
- Acknowledgement32564178993.Doc Final1Dokument6 SeitenAcknowledgement32564178993.Doc Final1Rashid AzmiNoch keine Bewertungen
- CHP 11 Moderate Nonskeletal Problems in Preadolescent ChildrenDokument6 SeitenCHP 11 Moderate Nonskeletal Problems in Preadolescent ChildrenJack Pai33% (3)
- Perioperative Management of AdrenalectomyDokument13 SeitenPerioperative Management of AdrenalectomyTJ LapuzNoch keine Bewertungen
- USMLE - VirusesDokument120 SeitenUSMLE - Viruseszeal7777100% (1)
- Sanjeevini Combination Sheet For SSC 8 Blood Pressure HighDokument1 SeiteSanjeevini Combination Sheet For SSC 8 Blood Pressure HighEduardoNoch keine Bewertungen
- Chessick - The Future of PsychoanalysisDokument283 SeitenChessick - The Future of Psychoanalysisuterw100% (1)
- Home Remedies Using Onion Prophet666Dokument2 SeitenHome Remedies Using Onion Prophet666Hussainz AliNoch keine Bewertungen
- Autonomic Control of The Heart Cardiovascular Reflexes Student Version (7) - 2Dokument27 SeitenAutonomic Control of The Heart Cardiovascular Reflexes Student Version (7) - 2Mohammed MoghavelehNoch keine Bewertungen
- Uniformity of Dosage UnitsDokument5 SeitenUniformity of Dosage UnitsJai MurugeshNoch keine Bewertungen
- Callyspongia SP Callyspongia SP: Identification of Antioxidant Compounds in The Sponge The SpongeDokument7 SeitenCallyspongia SP Callyspongia SP: Identification of Antioxidant Compounds in The Sponge The SpongeZulfajriNoch keine Bewertungen
- The - Utics and Control of Sheep and Goat Diseases, An Issue of Veterinary Clinics, Food Animal PracticeDokument262 SeitenThe - Utics and Control of Sheep and Goat Diseases, An Issue of Veterinary Clinics, Food Animal PracticeIurydyana Villalobos0% (1)
- Food Saftey PDFDokument22 SeitenFood Saftey PDFharsha vardhanNoch keine Bewertungen
- Biofeedback 2000x-Pert Hardware ManualDokument45 SeitenBiofeedback 2000x-Pert Hardware ManualNery BorgesNoch keine Bewertungen
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeVon EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeBewertung: 4.5 von 5 Sternen4.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsVon EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsBewertung: 4.5 von 5 Sternen4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (46)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (60)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsVon EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNoch keine Bewertungen
- Hearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIVon EverandHearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIBewertung: 4 von 5 Sternen4/5 (20)