Das könnte Ihnen auch gefallen
- Team ATG Standards (Ben Patrick)Dokument27 SeitenTeam ATG Standards (Ben Patrick)rodrigo vieira88% (8)
- Step 1: Reverse Out Knee PainDokument11 SeitenStep 1: Reverse Out Knee PainGrant Cherry100% (3)
- Jaegersports Jband ManualDokument16 SeitenJaegersports Jband Manualjosephmw0308Noch keine Bewertungen
- BJJ Roadmap 1.3Dokument35 SeitenBJJ Roadmap 1.3daviid93% (28)
- How to Dunk if You’re Under 6 Feet Tall - 13 Proven Ways to Jump Higher and Drastically Increase Your Vertical Jump in 4 WeeksVon EverandHow to Dunk if You’re Under 6 Feet Tall - 13 Proven Ways to Jump Higher and Drastically Increase Your Vertical Jump in 4 WeeksBewertung: 4 von 5 Sternen4/5 (2)
- 7 Patellar Tracking Exercises For Subluxation & DislocationDokument9 Seiten7 Patellar Tracking Exercises For Subluxation & DislocationAnh Đức NguyễnNoch keine Bewertungen
- Roadmap For BJJ Gold Ver 2.0 PDFDokument119 SeitenRoadmap For BJJ Gold Ver 2.0 PDFJarred L. Jasper100% (1)
- Wwe13 Wii OnlinemanDokument21 SeitenWwe13 Wii OnlinemanrockettekcorNoch keine Bewertungen
- Ultra Depth - The Most Astounding Hypnosis Discovery of Our TimeDokument6 SeitenUltra Depth - The Most Astounding Hypnosis Discovery of Our TimeHuib Salomons91% (11)
- HST Faq BookDokument132 SeitenHST Faq BookLucija Kosi100% (1)
- Beyond Grappling Technique GuideDokument18 SeitenBeyond Grappling Technique Guidefnavarretec8668100% (1)
- Psychology A New Introduction For A Level by Richard Gross, Rob Mcilveen, Hugh Coolican, Julia Russell, Alan ClampDokument944 SeitenPsychology A New Introduction For A Level by Richard Gross, Rob Mcilveen, Hugh Coolican, Julia Russell, Alan ClampSyeda Malika AnjumNoch keine Bewertungen
- Ben Greenfield Bulletproof Your Knee PDFDokument25 SeitenBen Greenfield Bulletproof Your Knee PDFhiggs1100% (1)
- Iron Gym Xtreme Work Out and Nutrition GuideDokument12 SeitenIron Gym Xtreme Work Out and Nutrition GuideEdwardKaNoch keine Bewertungen
- Free527 Vert Shock PDF Download Vertical Jump Trai - 59db17d91723dd898cdc3840Dokument2 SeitenFree527 Vert Shock PDF Download Vertical Jump Trai - 59db17d91723dd898cdc3840Johana Garcia0% (1)
- Help With Training For 1B, No Gym Available - Christian Thibaudeau Coaching - Forums - T NationDokument5 SeitenHelp With Training For 1B, No Gym Available - Christian Thibaudeau Coaching - Forums - T NationVladimir OlefirenkoNoch keine Bewertungen
- Crazy 8s Bodyweight CircuitsDokument16 SeitenCrazy 8s Bodyweight CircuitscavaleramaxNoch keine Bewertungen
- (Weis D.) BodyBuilding - Secret ExercisesDokument30 Seiten(Weis D.) BodyBuilding - Secret ExercisesMuhammad Ali Mukhtar100% (1)
- Krav Maga : Testing SyllabusDokument13 SeitenKrav Maga : Testing SyllabusMkhululiNoch keine Bewertungen
- Compartment SyndromeDokument66 SeitenCompartment Syndromeimammardani100% (1)
- Ring Training For Elite FitnessDokument0 SeitenRing Training For Elite FitnessZackary Thomas Gibbons71% (7)
- Leadership MGTDokument30 SeitenLeadership MGTJay-Dee Evangelista PacionNoch keine Bewertungen
- Ultimate Knee Guide For Getting Rid of Pain & Avoiding SurgeryVon EverandUltimate Knee Guide For Getting Rid of Pain & Avoiding SurgeryNoch keine Bewertungen
- Robert Melillo, Gerry Leisman (Auth.) - Neurobehavioral Disorders of Childhood - An Evolutionary Perspective (2010, Springer US)Dokument452 SeitenRobert Melillo, Gerry Leisman (Auth.) - Neurobehavioral Disorders of Childhood - An Evolutionary Perspective (2010, Springer US)santiago contrerasNoch keine Bewertungen
- Ball Exercise ChartDokument2 SeitenBall Exercise Chartsameet_aswaniNoch keine Bewertungen
- Booty Workout MadBarDokument12 SeitenBooty Workout MadBarCosmin Dospinescu100% (1)
- Achieving Structural Balance - Upper Body PushDokument22 SeitenAchieving Structural Balance - Upper Body Pushdjoiner45100% (5)
- Front Lever Tutorial 4ab8cfea A19b 4f83 A596 A22faf632941Dokument23 SeitenFront Lever Tutorial 4ab8cfea A19b 4f83 A596 A22faf632941jasoo__100% (6)
- 4 Weeks To Bigger Legs - T NationDokument33 Seiten4 Weeks To Bigger Legs - T NationCALFNoch keine Bewertungen
- 5 Most Common Yoga Injuries (And How You Can Avoid Them)Von Everand5 Most Common Yoga Injuries (And How You Can Avoid Them)Noch keine Bewertungen
- GMAU Krav Maga Testing SyllabusDokument13 SeitenGMAU Krav Maga Testing SyllabusJulio OlmedoNoch keine Bewertungen
- What Do You All Think of Kneesovertoesguy - Are His Exercises Useful For Judokas in Your Opinions - JudoDokument3 SeitenWhat Do You All Think of Kneesovertoesguy - Are His Exercises Useful For Judokas in Your Opinions - JudoAbbas RazaNoch keine Bewertungen
- Roadmap For BJJ 1.4 PDFDokument34 SeitenRoadmap For BJJ 1.4 PDFkaman3000Noch keine Bewertungen
- Escala FAOS IAPTDokument6 SeitenEscala FAOS IAPTRui Pedro SantiagoNoch keine Bewertungen
- HAGOSenglishDokument5 SeitenHAGOSenglishjavierNoch keine Bewertungen
- Student Hip 2015Dokument8 SeitenStudent Hip 2015Anonymous JhEds4Noch keine Bewertungen
- IT Band StretchesDokument1 SeiteIT Band StretchesMark MooreNoch keine Bewertungen
- Oxford Knee ScoreDokument3 SeitenOxford Knee ScoreAnna Maria Cristina RaduNoch keine Bewertungen
- Testing: Discounts & Deals - S U!Dokument8 SeitenTesting: Discounts & Deals - S U!D Vinay KumarNoch keine Bewertungen
- 6 7 Weekly Exercises You Can't Skip - Bigger StrongDokument9 Seiten6 7 Weekly Exercises You Can't Skip - Bigger StrongjesseNoch keine Bewertungen
- Captura de Pantalla 2024-04-02 A La(s) 8.39.32 A.M.Dokument106 SeitenCaptura de Pantalla 2024-04-02 A La(s) 8.39.32 A.M.fernandaduronNoch keine Bewertungen
- O o o o o o o o O: Home Contact UsDokument4 SeitenO o o o o o o o O: Home Contact UsshaneNoch keine Bewertungen
- CableCross ExercisesDokument8 SeitenCableCross ExercisesGustavo CabanasNoch keine Bewertungen
- Faos Foot & Ankle Survey: InstructionsDokument4 SeitenFaos Foot & Ankle Survey: InstructionsShah12Noch keine Bewertungen
- Coastal Iliotibial Band 2014Dokument2 SeitenCoastal Iliotibial Band 2014lesterbsbNoch keine Bewertungen
- The Turkish Get-Up, Part 3: Overhead Squat VariationDokument3 SeitenThe Turkish Get-Up, Part 3: Overhead Squat VariationHONGJYNoch keine Bewertungen
- Booty Workout PDFDokument12 SeitenBooty Workout PDFjasoo__Noch keine Bewertungen
- PTMSK Case Write Up Example 2Dokument8 SeitenPTMSK Case Write Up Example 2Tan Zhen XinNoch keine Bewertungen
- Helping To Solve Fitting ProblemsDokument6 SeitenHelping To Solve Fitting ProblemsgonvazNoch keine Bewertungen
- Doorway Pull Up Bar, Strength Training Pull-Up Door Frame Bars, Total Upper Body Workout Bar For Doorway With FoamDokument1 SeiteDoorway Pull Up Bar, Strength Training Pull-Up Door Frame Bars, Total Upper Body Workout Bar For Doorway With FoamJerome WhyteNoch keine Bewertungen
- Clinical Examination of The Lower Leg, Ankle and Foot: HistoryDokument9 SeitenClinical Examination of The Lower Leg, Ankle and Foot: HistoryJanhvi AswaniNoch keine Bewertungen
- The Fabulous 15 Top 15 Exercises For Higher Vertical Jumps - DeFranco's TrainingDokument6 SeitenThe Fabulous 15 Top 15 Exercises For Higher Vertical Jumps - DeFranco's Trainingdr_finch511Noch keine Bewertungen
- Thumb Spica Splint BootsDokument1 SeiteThumb Spica Splint Bootsjdavies231Noch keine Bewertungen
- Achieving Structural BalanceDokument8 SeitenAchieving Structural Balancesebastian bowringNoch keine Bewertungen
- The Ultimate Guide To Improving Joint MobilityDokument9 SeitenThe Ultimate Guide To Improving Joint MobilityVladimir CocaNoch keine Bewertungen
- Biceps Brachii TestDokument1 SeiteBiceps Brachii TestFlorin ArdeleanuNoch keine Bewertungen
- 8 Week Workout ProgrammeDokument17 Seiten8 Week Workout ProgrammeOossNoch keine Bewertungen
- Improving Balance For Daily Life and Sport - StrongFirstDokument9 SeitenImproving Balance For Daily Life and Sport - StrongFirstPa BloNoch keine Bewertungen
- Study Guide Questions: 9.4: Assessment, 6Dokument7 SeitenStudy Guide Questions: 9.4: Assessment, 6api-502504563Noch keine Bewertungen
- 9better Than The Barbell Row - Bigger Stronger LeaDokument6 Seiten9better Than The Barbell Row - Bigger Stronger LeajesseNoch keine Bewertungen
- Consequences of Not SquattingDokument740 SeitenConsequences of Not SquattingPankaj SharmaNoch keine Bewertungen
- Knee Injury and Osteoarthritis Outcome Score Koos PDFDokument4 SeitenKnee Injury and Osteoarthritis Outcome Score Koos PDFNuruel Thamie PoethreeNoch keine Bewertungen
- What's This Shoe All About?: Changing People's Lives and Much More!Von EverandWhat's This Shoe All About?: Changing People's Lives and Much More!Noch keine Bewertungen
- 1Dokument27 Seiten1Lucija KosiNoch keine Bewertungen
- Offensive Offensive/Defensive Defensive Miscellaneous: Sorcerer SpellsDokument1 SeiteOffensive Offensive/Defensive Defensive Miscellaneous: Sorcerer SpellsLucija KosiNoch keine Bewertungen
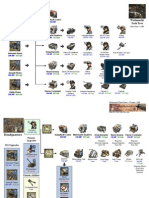
- Headquarters: Werhmacht Tech TreeDokument10 SeitenHeadquarters: Werhmacht Tech TreeLucija KosiNoch keine Bewertungen
- PETechTreev2 300Dokument9 SeitenPETechTreev2 300Lucija KosiNoch keine Bewertungen
- This Goal Coupled With The REFLECT Approach That Government HasDokument3 SeitenThis Goal Coupled With The REFLECT Approach That Government Hasmuna moonoNoch keine Bewertungen
- JCR 2008 Soc SC EditionDokument196 SeitenJCR 2008 Soc SC Editionasifch_lumsNoch keine Bewertungen
- Inventory EvidenceDokument21 SeitenInventory Evidenceapi-548178934Noch keine Bewertungen
- Nursing Process EBN Format OB PEDIADokument5 SeitenNursing Process EBN Format OB PEDIAAnn Nicole UlitNoch keine Bewertungen
- Positivitrees LessonDokument5 SeitenPositivitrees Lessonapi-380331542Noch keine Bewertungen
- English 8 Q1 M2 W2,3Dokument20 SeitenEnglish 8 Q1 M2 W2,3Ericzon SantosNoch keine Bewertungen
- Letter of Dissolution Author(s) : Jacques Lacan and Jeffrey Mehlman Source: October, Vol. 40, Television (Spring, 1987), Pp. 128-130 Published By: The MIT Press Accessed: 10-06-2020 15:50 UTCDokument4 SeitenLetter of Dissolution Author(s) : Jacques Lacan and Jeffrey Mehlman Source: October, Vol. 40, Television (Spring, 1987), Pp. 128-130 Published By: The MIT Press Accessed: 10-06-2020 15:50 UTCMohamed TalNoch keine Bewertungen
- Online or Digital Learning: Xienicxel A. GalangDokument3 SeitenOnline or Digital Learning: Xienicxel A. GalangPrincess Sam LiwagNoch keine Bewertungen
- American Indian Family PatternsDokument11 SeitenAmerican Indian Family PatternsRobin KeatingNoch keine Bewertungen
- Topic 5Dokument3 SeitenTopic 5Yuki BarracaNoch keine Bewertungen
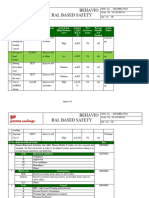
- BBS - Risk - Assessment UpdatedDokument2 SeitenBBS - Risk - Assessment UpdatedSuraj RawatNoch keine Bewertungen
- Greenwood. H. 2012. What Aspects of An Art Therapy Group Aid Recovery For People Diagnosed With PsychosisDokument32 SeitenGreenwood. H. 2012. What Aspects of An Art Therapy Group Aid Recovery For People Diagnosed With PsychosisIssy MitchellNoch keine Bewertungen
- Informative Speech - Gwyneth GloriosoDokument3 SeitenInformative Speech - Gwyneth Gloriosoapi-533577985Noch keine Bewertungen
- Clinical Nursing JudgmentDokument6 SeitenClinical Nursing Judgmentapi-662695034Noch keine Bewertungen
- PB Xii Eng Core.2023-24Dokument14 SeitenPB Xii Eng Core.2023-24everythingisgonnabeallright007100% (1)
- Importance of Friends in Our LivesDokument3 SeitenImportance of Friends in Our LivesMuhammad FarhanNoch keine Bewertungen
- (Edited) N31-G6-SOP-and-Conceptual-FrameworkDokument5 Seiten(Edited) N31-G6-SOP-and-Conceptual-Frameworkst michael machine shopNoch keine Bewertungen
- Skill AssignmentDokument2 SeitenSkill AssignmentSuryaNoch keine Bewertungen
- MODULE # 13 AssignmentDokument12 SeitenMODULE # 13 AssignmentMarjorie BaculioNoch keine Bewertungen
- Understanding Mental HealthDokument6 SeitenUnderstanding Mental Healthmayorking11Noch keine Bewertungen
- Imogene KingDokument16 SeitenImogene KingIsabel HernandezNoch keine Bewertungen
- University Institute of Legal Studies Department of LawDokument12 SeitenUniversity Institute of Legal Studies Department of LawHarneet KaurNoch keine Bewertungen
- The Bureau of Jail Management and Penology (BJMP) : Jojo P. Bautista, MscrimDokument38 SeitenThe Bureau of Jail Management and Penology (BJMP) : Jojo P. Bautista, MscrimBonn Allen Christopher VictorianoNoch keine Bewertungen
- JH Fall Risk Assessment ToolDokument1 SeiteJH Fall Risk Assessment ToolMaria SantiagoNoch keine Bewertungen
- Review of Related LiteratureDokument3 SeitenReview of Related LiteratureJake CuencyNoch keine Bewertungen
- 4th quarterEnglish9PretestDokument5 Seiten4th quarterEnglish9PretestPauline Diane PresenteNoch keine Bewertungen