Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDokument1 SeiteInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanNoch keine Bewertungen
- Investigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Dokument1 SeiteInvestigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Andy DolmanNoch keine Bewertungen
- PSM Investigation Compliance ChecklistDokument1 SeitePSM Investigation Compliance ChecklistAndy DolmanNoch keine Bewertungen
- Incident InvestDokument1 SeiteIncident InvestAndy DolmanNoch keine Bewertungen
- Investigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoDokument1 SeiteInvestigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoAndy DolmanNoch keine Bewertungen
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDokument1 SeiteInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanNoch keine Bewertungen
- Sample Investigation Improvement Checklist Incident Investigation GuidelineDokument2 SeitenSample Investigation Improvement Checklist Incident Investigation GuidelineAndy DolmanNoch keine Bewertungen
- Investigator Name: Event Assessed: Date of AssessmentDokument1 SeiteInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanNoch keine Bewertungen
- Checklist For Developing An Incident Investigation PlanDokument1 SeiteChecklist For Developing An Incident Investigation PlanAndy DolmanNoch keine Bewertungen
- Incident InvestDokument1 SeiteIncident InvestAndy DolmanNoch keine Bewertungen
- Sample Formal Report Outline Incident Investigation GuidelineDokument1 SeiteSample Formal Report Outline Incident Investigation GuidelineAndy DolmanNoch keine Bewertungen
- Flashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Dokument8 SeitenFlashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Andy DolmanNoch keine Bewertungen
- Comprehensive List of CausesDokument1 SeiteComprehensive List of CausesAndy DolmanNoch keine Bewertungen
- Quick Checklist For Investigators: Physical ItemsDokument4 SeitenQuick Checklist For Investigators: Physical ItemsAndy DolmanNoch keine Bewertungen
- Investigator Name: Event Assessed: Date of AssessmentDokument1 SeiteInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanNoch keine Bewertungen
- Customize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationDokument4 SeitenCustomize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationAndy DolmanNoch keine Bewertungen
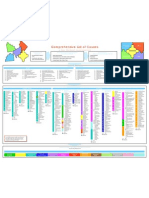
- Propane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Dokument2 SeitenPropane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Andy DolmanNoch keine Bewertungen
- Checklist To Prepare For An Inspection Incident Investigation GuidelineDokument1 SeiteChecklist To Prepare For An Inspection Incident Investigation GuidelineAndy DolmanNoch keine Bewertungen
- Incident InvestDokument5 SeitenIncident InvestAndy DolmanNoch keine Bewertungen
- Incident InvestDokument16 SeitenIncident InvestAndy DolmanNoch keine Bewertungen
- Appendix F: Selected OSHA and EPA Incident Investigation RegulationsDokument3 SeitenAppendix F: Selected OSHA and EPA Incident Investigation RegulationsAndy DolmanNoch keine Bewertungen
- Quick checklist for incident investigatorsDokument5 SeitenQuick checklist for incident investigatorsAndy DolmanNoch keine Bewertungen
- Relevant Organizations GuideDokument3 SeitenRelevant Organizations GuideAndy DolmanNoch keine Bewertungen
- Appendix C: Photography Guidelines For Maximum ResultsDokument3 SeitenAppendix C: Photography Guidelines For Maximum ResultsAndy DolmanNoch keine Bewertungen
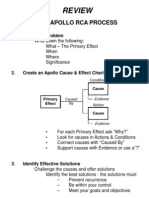
- Review: The Apollo Rca ProcessDokument1 SeiteReview: The Apollo Rca ProcessAndy DolmanNoch keine Bewertungen
- Incident InvestDokument21 SeitenIncident InvestAndy DolmanNoch keine Bewertungen
- Appendix B: Professional Assistance DirectoryDokument2 SeitenAppendix B: Professional Assistance DirectoryAndy DolmanNoch keine Bewertungen
- Continuous Improvement For The Incident Investigation SystemDokument10 SeitenContinuous Improvement For The Incident Investigation SystemAndy DolmanNoch keine Bewertungen
- Incident InvestDokument17 SeitenIncident InvestAndy DolmanNoch keine Bewertungen
- Incident InvestDokument17 SeitenIncident InvestAndy DolmanNoch keine Bewertungen