Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Euromonitor International - Analysis ArgentinaDokument2 SeitenEuromonitor International - Analysis ArgentinamqcpiqmsNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- CSC Accredited Private Training Institutions (ATI)Dokument18 SeitenCSC Accredited Private Training Institutions (ATI)mqcpiqmsNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Social Studies Reviewer Part 1Dokument10 SeitenSocial Studies Reviewer Part 1mqcpiqms0% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Non-Deped Schools Issued A Provisional Permit For Sy 2015-2016 As of April 9, 2015Dokument47 SeitenNon-Deped Schools Issued A Provisional Permit For Sy 2015-2016 As of April 9, 2015mqcpiqmsNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Session 7 - Theory of ProductionDokument28 SeitenSession 7 - Theory of ProductionmqcpiqmsNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Policy On Inter Office Communication 1st EditionDokument10 SeitenPolicy On Inter Office Communication 1st Editionmqcpiqms100% (1)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Session 8 - Theory of Cost and ProfitDokument7 SeitenSession 8 - Theory of Cost and ProfitmqcpiqmsNoch keine Bewertungen
- Ashoka University CurriculumDokument11 SeitenAshoka University CurriculumAnjana MadhavanNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- CV Wael Haddoush Eng.Dokument3 SeitenCV Wael Haddoush Eng.Anonymous JEydS3QIgfNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- SE - Test Clear - 2106Dokument3 SeitenSE - Test Clear - 2106Vatsalya AhujaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
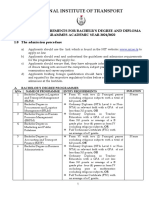
- National Institute of TransportDokument7 SeitenNational Institute of TransportSele BreezeNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- UToronto UG 2022 23Dokument19 SeitenUToronto UG 2022 23PaolaNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
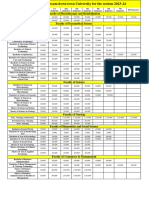
- Fees Structure Assam Down Town University For The Session 2023 2Dokument2 SeitenFees Structure Assam Down Town University For The Session 2023 2Debashish SharmaNoch keine Bewertungen
- A5 Broschure General Information 1412Dokument60 SeitenA5 Broschure General Information 1412Olivia HeckelNoch keine Bewertungen
- PG Bag Soss eDokument105 SeitenPG Bag Soss eDIVYANSH SAHU BA LLB (HONOURS)Noch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Geothermal Institute BrochureDokument8 SeitenGeothermal Institute BrochureJakechris SicadNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Ayurveda Final MseDokument43 SeitenAyurveda Final MseMikel MillerNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- 2 JHA Capital University JharkhandDokument6 Seiten2 JHA Capital University JharkhandDigital DynamicNoch keine Bewertungen
- Education System Bangladesh PDFDokument15 SeitenEducation System Bangladesh PDFmohitgarg08Noch keine Bewertungen
- M.S.A. - FitDokument3 SeitenM.S.A. - FitJunior Mebude SimbaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Catalog10 11Dokument241 SeitenCatalog10 11vsinisa1Noch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Monograph FormatDokument20 SeitenMonograph FormatRahman Aqa100% (1)
- Ferdinand San Buenaventura. Sir SolDokument6 SeitenFerdinand San Buenaventura. Sir SolDenand Abaya San BuenaventuraNoch keine Bewertungen
- (Appendix 2A) RPMS Tool For Proficient Teacher-Broadcasters SY 2021-2022 in The Time of COVID-19Dokument27 Seiten(Appendix 2A) RPMS Tool For Proficient Teacher-Broadcasters SY 2021-2022 in The Time of COVID-19Nino IgnacioNoch keine Bewertungen
- NALSAR Prospectus - MergedDokument17 SeitenNALSAR Prospectus - MergedSAMBITPRIYADARSHINoch keine Bewertungen
- Haas Recruit05Dokument16 SeitenHaas Recruit05chienNoch keine Bewertungen
- SLU MLSP ATS QuestionnaireDokument8 SeitenSLU MLSP ATS QuestionnaireOdyNoch keine Bewertungen
- Architecture Nationaly Harmonized Curriculum 2017Dokument231 SeitenArchitecture Nationaly Harmonized Curriculum 2017tegbaruNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- CHED Strategic Plan 2017-2022 As of Nov 27, 2017 With TablesDokument50 SeitenCHED Strategic Plan 2017-2022 As of Nov 27, 2017 With TablesJoselito Alisuag93% (41)
- Application Form Punjab Social Security Health Management Company (Model Town 30-E/3, Lahore)Dokument1 SeiteApplication Form Punjab Social Security Health Management Company (Model Town 30-E/3, Lahore)musaddiq islamNoch keine Bewertungen
- 1647 Accreditation Report NSKU Ba Instrument Engineering 2013-09-27Dokument71 Seiten1647 Accreditation Report NSKU Ba Instrument Engineering 2013-09-27muhammad bilalNoch keine Bewertungen
- Advt No 1 2015Dokument10 SeitenAdvt No 1 2015sapna24Noch keine Bewertungen
- PS Early Childhood Education BIDokument83 SeitenPS Early Childhood Education BIManja125Noch keine Bewertungen
- COUN ED HandbookDokument50 SeitenCOUN ED HandbookCSUFCounselorEdNoch keine Bewertungen
- Sampoerna UniversityDokument6 SeitenSampoerna Universitysuzie halimaNoch keine Bewertungen
- Ahmed Lashin PortfolioDokument244 SeitenAhmed Lashin PortfolioAhmed LashinNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)