Das könnte Ihnen auch gefallen
- IFMA Product ManualDokument8 SeitenIFMA Product ManualIbnu AndhikaNoch keine Bewertungen
- Maxiforce 2009 CatalogDokument228 SeitenMaxiforce 2009 CatalogMotokoy Sprekitik Takoykoy100% (1)
- Fluke 725 Multifunction CalibratorDokument1 SeiteFluke 725 Multifunction CalibratorAdrianzzzzNoch keine Bewertungen
- PLC Programming Course1 KMXDokument55 SeitenPLC Programming Course1 KMXtitohemanNoch keine Bewertungen
- 0900-9914 I1 201012Dokument132 Seiten0900-9914 I1 201012carlosj_echeverria100% (1)
- Bigblue400cxce (Lj140121e)Dokument88 SeitenBigblue400cxce (Lj140121e)masswelding ingenieriaNoch keine Bewertungen
- Service ManualDokument332 SeitenService ManualfalcoNoch keine Bewertungen
- Big Blue Air PakDokument146 SeitenBig Blue Air Pakhidayat rachmatNoch keine Bewertungen
- Linkoln Ranger 300 DLXDokument56 SeitenLinkoln Ranger 300 DLXkarimNoch keine Bewertungen
- As 71745 FD-Q Im 96M13515 GB WW 1086-3Dokument10 SeitenAs 71745 FD-Q Im 96M13515 GB WW 1086-3Ryan WilliamsNoch keine Bewertungen
- NBK V Pulley Rev 3Dokument14 SeitenNBK V Pulley Rev 3Ferry KurniaNoch keine Bewertungen
- Toor Complaint DocumentDokument5 SeitenToor Complaint DocumentbolankimNoch keine Bewertungen
- LIT2299 Rev 10 PD12C Parts ListDokument28 SeitenLIT2299 Rev 10 PD12C Parts ListYuliana Andrea Zapata RubioNoch keine Bewertungen
- MC 10115469 9999Dokument6 SeitenMC 10115469 9999Carlos YuliNoch keine Bewertungen
- NAVEDTRA 14050A Construction Mechanic Advanced Part 2 PDFDokument170 SeitenNAVEDTRA 14050A Construction Mechanic Advanced Part 2 PDFChris MilonasNoch keine Bewertungen
- Tool List: Please Read Completely Before BeginningDokument5 SeitenTool List: Please Read Completely Before BeginningDavíð Örn SvavarssonNoch keine Bewertungen
- MEP 003A Intermediate and Depot Level Maintenance Manual TM 5 6115 585 34Dokument192 SeitenMEP 003A Intermediate and Depot Level Maintenance Manual TM 5 6115 585 34GreenMountainGeneratorsNoch keine Bewertungen
- Miller 198449 BoardDokument80 SeitenMiller 198449 BoardMario Emilio Castro TineoNoch keine Bewertungen
- LW Sparepart Lw450eDokument59 SeitenLW Sparepart Lw450eMatthew100% (1)
- Hastings PDFDokument220 SeitenHastings PDFEmily BullockNoch keine Bewertungen
- No Pipe Modification Necessary: Clamp-On Flow SensorDokument20 SeitenNo Pipe Modification Necessary: Clamp-On Flow SensorSaravanan VNoch keine Bewertungen
- Letter of ProxyDokument1 SeiteLetter of ProxyMitul Sayed Ashraf MamunNoch keine Bewertungen
- Bactron BiocideDokument175 SeitenBactron BiocideWell Lojumin100% (2)
- All-Track Service: AT-80HD Operator ManualDokument28 SeitenAll-Track Service: AT-80HD Operator ManualDavid OrtegaNoch keine Bewertungen
- Driven Point WellsDokument16 SeitenDriven Point WellsGabriela Patricia Flores AvilésNoch keine Bewertungen
- EMCO Large Engine Catalog 2008Dokument137 SeitenEMCO Large Engine Catalog 2008Robert KirkNoch keine Bewertungen
- 4 X 5 and 5 X 6 Parts & Service Manual TUL-C-600 - A PDFDokument47 Seiten4 X 5 and 5 X 6 Parts & Service Manual TUL-C-600 - A PDFzachNoch keine Bewertungen
- Model m75 Service ManualDokument40 SeitenModel m75 Service ManualMuhamad Sharif Bin ZainudinNoch keine Bewertungen
- Diesel Trade Theory n3 Aug QP 2019Dokument6 SeitenDiesel Trade Theory n3 Aug QP 2019Dennis MbegabolaweNoch keine Bewertungen
- Manual VP7D25 enDokument136 SeitenManual VP7D25 enDarbar JiNoch keine Bewertungen
- PISTON ENGINE GeneralupdatedDokument27 SeitenPISTON ENGINE GeneralupdatedSamarth SNoch keine Bewertungen
- Manual 000004336Dokument19 SeitenManual 000004336ridho_kresnaNoch keine Bewertungen
- TD8600005733 03e PDFDokument93 SeitenTD8600005733 03e PDFshahnamNoch keine Bewertungen
- Labrie - Heavy Duty Right-Hand Arm - Parts Manual - 90418Dokument42 SeitenLabrie - Heavy Duty Right-Hand Arm - Parts Manual - 90418stainless31620039126Noch keine Bewertungen
- Lincoln Ranger 305dDokument52 SeitenLincoln Ranger 305dAnibal Fabian GonzalezNoch keine Bewertungen
- Shema Esab Origo Mag C171 C201 C251Dokument20 SeitenShema Esab Origo Mag C171 C201 C251cornelutsNoch keine Bewertungen
- JT30AT Operator Manual (3152)Dokument243 SeitenJT30AT Operator Manual (3152)Luke FosterNoch keine Bewertungen
- VAG HYsec Hydraulic Brake and Lift UnitDokument3 SeitenVAG HYsec Hydraulic Brake and Lift UnitLuka Borna100% (1)
- Air Compressor For Scba - Type LW 100 e & LW 100 BDokument55 SeitenAir Compressor For Scba - Type LW 100 e & LW 100 BEserNoch keine Bewertungen
- Kobelt Module 7173 Manual PDFDokument21 SeitenKobelt Module 7173 Manual PDFDepil DepikaNoch keine Bewertungen
- Technical Proposal ECrane 1000 Series EH7359Dokument16 SeitenTechnical Proposal ECrane 1000 Series EH7359Satrio Agung WijonarkoNoch keine Bewertungen
- Ko Belt Steering GuideDokument37 SeitenKo Belt Steering GuideJorgelino ParkerNoch keine Bewertungen
- Tapers and Taper TurningDokument4 SeitenTapers and Taper TurningSayanSanyalNoch keine Bewertungen
- Test PDFDokument481 SeitenTest PDFHung Hua NhuNoch keine Bewertungen
- Lifting MechanismDokument14 SeitenLifting MechanismEWERTONNoch keine Bewertungen
- Catalogo de Antenas DiamondDokument7 SeitenCatalogo de Antenas DiamondEnder Ramirez100% (1)
- Arc MasterDokument60 SeitenArc MasterAbood AliNoch keine Bewertungen
- Trimble SPS 855Dokument5 SeitenTrimble SPS 855Alwin SyahperdanaNoch keine Bewertungen
- LIT2319 R4 CH175 Service ManualDokument40 SeitenLIT2319 R4 CH175 Service ManualAlfred HitchcockNoch keine Bewertungen
- Focs Plus Ldw1003 - GBDokument4 SeitenFocs Plus Ldw1003 - GBRafael LopezNoch keine Bewertungen
- ECO 410 DG Index A PDFDokument127 SeitenECO 410 DG Index A PDFKaren Baker100% (1)
- Accu Turn Manual 8944 Lathe W Parts ListDokument38 SeitenAccu Turn Manual 8944 Lathe W Parts ListJohnfromFresno100% (1)
- JT920 JT920C Parts Manual 053-467 PDFDokument284 SeitenJT920 JT920C Parts Manual 053-467 PDFRohammed CastilloNoch keine Bewertungen
- Technical Service Manual: Section TSM 144 1 of 10 Issue DDokument10 SeitenTechnical Service Manual: Section TSM 144 1 of 10 Issue DHector_Cornejo_5673Noch keine Bewertungen
- LD430c TroubleshootingDokument136 SeitenLD430c TroubleshootingGilberto IbarraNoch keine Bewertungen
- Fluke CatalogDokument164 SeitenFluke CatalogCharles BenwariNoch keine Bewertungen
- COHP FamilyDokument4 SeitenCOHP FamilyAbigail Aracely Ochoa AlvaradoNoch keine Bewertungen
- Sedgwick Logo - Certification of Health Care Provider For Family Member's Serious Health Condition (FMLA)Dokument4 SeitenSedgwick Logo - Certification of Health Care Provider For Family Member's Serious Health Condition (FMLA)teamirNoch keine Bewertungen
- WH 380 eDokument4 SeitenWH 380 ePor Justica EN YumaNoch keine Bewertungen
- SRD Insurance and Billing Practices 2020 DoneDokument3 SeitenSRD Insurance and Billing Practices 2020 DoneAndy WilsonNoch keine Bewertungen
- LG Main CoreDokument1 SeiteLG Main CoreAndy WilsonNoch keine Bewertungen
- SRD Minor Patient Consent To Treatment 2020 DoneDokument1 SeiteSRD Minor Patient Consent To Treatment 2020 DoneAndy WilsonNoch keine Bewertungen
- Back Assessment Reassessment Handbook August 2012Dokument18 SeitenBack Assessment Reassessment Handbook August 2012Andy WilsonNoch keine Bewertungen
- CRT TV Sign CrapDokument1 SeiteCRT TV Sign CrapAndy WilsonNoch keine Bewertungen
- Disassembly Monito 20106122290Dokument33 SeitenDisassembly Monito 20106122290Andy WilsonNoch keine Bewertungen
- Tennessee LawDokument13 SeitenTennessee LawAndy WilsonNoch keine Bewertungen
- Aluminum Electrolytic Capacitors SMTDokument5 SeitenAluminum Electrolytic Capacitors SMTAndy WilsonNoch keine Bewertungen
- Samsung HLS5697S MainDokument3 SeitenSamsung HLS5697S MainAndy WilsonNoch keine Bewertungen
- 51PP9200 PDFDokument166 Seiten51PP9200 PDFAndy WilsonNoch keine Bewertungen
- Agc On Acu BrochureDokument2 SeitenAgc On Acu BrochureAndy WilsonNoch keine Bewertungen
- Adkins WorkorderDokument2 SeitenAdkins WorkorderAndy WilsonNoch keine Bewertungen
- Img 0006Dokument6 SeitenImg 0006Andy WilsonNoch keine Bewertungen
- Philips 42 Inch LCD Power Ic-Fsq510Dokument14 SeitenPhilips 42 Inch LCD Power Ic-Fsq510Raja Pathamuthu.GNoch keine Bewertungen
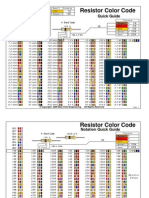
- Resistencias Codigo Colores PDFDokument2 SeitenResistencias Codigo Colores PDF'Cesar Guel81% (16)
- HL67A750 Firmware Update InstructionDokument6 SeitenHL67A750 Firmware Update InstructionAndy WilsonNoch keine Bewertungen
- Basic LCD TV Trouble Shooting Guide by Bud MartinDokument9 SeitenBasic LCD TV Trouble Shooting Guide by Bud MartinJustin WilliamsNoch keine Bewertungen
- LJ41 05120aDokument1 SeiteLJ41 05120aAndy WilsonNoch keine Bewertungen
- Reception Maps GuideDokument1 SeiteReception Maps GuideAndy WilsonNoch keine Bewertungen
- HL67A750 Firmware Update InstructionDokument6 SeitenHL67A750 Firmware Update InstructionAndy WilsonNoch keine Bewertungen
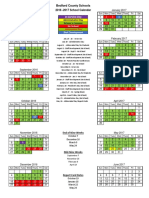
- Bedford County Schools: 2016 - 2017 School CalendarDokument1 SeiteBedford County Schools: 2016 - 2017 School CalendarAndy WilsonNoch keine Bewertungen
- Firmware Update Panasonic Tc-pxxst30 Gt30 Vt30 Pst34 Dt30 v222 InstallationDokument6 SeitenFirmware Update Panasonic Tc-pxxst30 Gt30 Vt30 Pst34 Dt30 v222 InstallationAndy WilsonNoch keine Bewertungen
- Philips CDR760 17 Dfu AenDokument54 SeitenPhilips CDR760 17 Dfu AenAndy WilsonNoch keine Bewertungen
- Bedford County Schools: 2016 - 2017 School CalendarDokument1 SeiteBedford County Schools: 2016 - 2017 School CalendarAndy WilsonNoch keine Bewertungen
- Privacy in The WorkplaceDokument16 SeitenPrivacy in The WorkplaceAndy WilsonNoch keine Bewertungen
- Philips 42 Inch LCD Power Ic-Fsq510Dokument14 SeitenPhilips 42 Inch LCD Power Ic-Fsq510Raja Pathamuthu.GNoch keine Bewertungen
- Who Must Register ChartDokument1 SeiteWho Must Register ChartAndy WilsonNoch keine Bewertungen
- CTAS Sunshine Law 2016Dokument11 SeitenCTAS Sunshine Law 2016Andy Wilson100% (1)
- LCD Lamp CrossDokument16 SeitenLCD Lamp CrossAndy WilsonNoch keine Bewertungen
- Fasco Full Catalog PDFDokument184 SeitenFasco Full Catalog PDFvickersNoch keine Bewertungen
- Om Prakash vs. State of Rajasthan ANRDokument10 SeitenOm Prakash vs. State of Rajasthan ANRTalluri RambabuNoch keine Bewertungen
- Peace and Order and Public Safety PlanDokument3 SeitenPeace and Order and Public Safety PlanTurado JaniceNoch keine Bewertungen
- Ethical Issues in Qualitative Research PDFDokument2 SeitenEthical Issues in Qualitative Research PDFJennaNoch keine Bewertungen
- Oposa Vs Factoran DigestDokument2 SeitenOposa Vs Factoran Digestjireh100% (1)
- HandOuts For John of SalisburyDokument3 SeitenHandOuts For John of SalisburyMelchizedek Beton OmandamNoch keine Bewertungen
- Elementary Principles of EconomicsDokument546 SeitenElementary Principles of EconomicssowmyabpNoch keine Bewertungen
- Deloitte NL Risk Compliance Risk AssessmentsDokument8 SeitenDeloitte NL Risk Compliance Risk AssessmentsEwan PowrieNoch keine Bewertungen
- Legal MethodDokument23 SeitenLegal Methodnayan96.mdgrNoch keine Bewertungen
- 09 Some Problems of Comparative PhilosophyDokument5 Seiten09 Some Problems of Comparative PhilosophyGediminas GiedraitisNoch keine Bewertungen
- Miss Sarah Sampson Act III Scenes 1 and 2 - Gotthold Ephraim LessingDokument8 SeitenMiss Sarah Sampson Act III Scenes 1 and 2 - Gotthold Ephraim LessingJennie PardoeNoch keine Bewertungen
- Erp Treatment Paper SalkovskisDokument5 SeitenErp Treatment Paper SalkovskisMyraChNoch keine Bewertungen
- Module 2 Asking Good Questions Empathy Confrontation Hand OutDokument62 SeitenModule 2 Asking Good Questions Empathy Confrontation Hand OutReilpeterNoch keine Bewertungen
- Aquino Administration and The Bill of RightsDokument2 SeitenAquino Administration and The Bill of RightsAndrea Hana DevezaNoch keine Bewertungen
- Desmet 2013 PositiveDesignAnIntroductiontoDesignforSubjectiveWell Being TRADDokument15 SeitenDesmet 2013 PositiveDesignAnIntroductiontoDesignforSubjectiveWell Being TRADCosta HumbertoNoch keine Bewertungen
- Project LawDokument72 SeitenProject LawKapildev DhakaNoch keine Bewertungen
- DatanomicsDokument3 SeitenDatanomicsOscar JaraNoch keine Bewertungen
- ATESTAT Engleză FINALpdfDokument27 SeitenATESTAT Engleză FINALpdfFlavia Munteanu100% (1)
- Ramadan Employee GuideDokument12 SeitenRamadan Employee GuideRoubwezNoch keine Bewertungen
- Ferraris v. FerrarisDokument2 SeitenFerraris v. FerrarisTrix BermosaNoch keine Bewertungen
- Aristotle "Poetics": Aspects of Aristotle "Poetics" in Modern LiteratureDokument7 SeitenAristotle "Poetics": Aspects of Aristotle "Poetics" in Modern LiteratureVikram Mishra100% (1)
- Locus Standi in Company LawDokument3 SeitenLocus Standi in Company LawlucindaNoch keine Bewertungen
- Lost at Sea 1.WKBDokument9 SeitenLost at Sea 1.WKBسلطان مغلNoch keine Bewertungen
- Group Policy 1. INTRODUCTION 2. BUSINESS INTEGRITY. 2.1. Honesty, Integrity & FairnessDokument11 SeitenGroup Policy 1. INTRODUCTION 2. BUSINESS INTEGRITY. 2.1. Honesty, Integrity & FairnessbojaNoch keine Bewertungen
- Plagiarism Preventio PolicyDokument30 SeitenPlagiarism Preventio PolicyParan GoswamiNoch keine Bewertungen
- Forensic ThesisDokument38 SeitenForensic ThesisZivi DegenNoch keine Bewertungen
- Dominica Constitution Part OneDokument5 SeitenDominica Constitution Part OneTyron BenjaminNoch keine Bewertungen
- Doyle V Board of Executors (Trust Beneficiary Rigths)Dokument1 SeiteDoyle V Board of Executors (Trust Beneficiary Rigths)jNoch keine Bewertungen
- Aswer Philo ExamDokument3 SeitenAswer Philo ExamBETHUEL P. ALQUIROZNoch keine Bewertungen
- Overall Guidelines For Iap Applicants: Funding For Up ToDokument8 SeitenOverall Guidelines For Iap Applicants: Funding For Up Toabel_kayelNoch keine Bewertungen
- Value Education Study Notes: Non-Core SubjectsDokument27 SeitenValue Education Study Notes: Non-Core Subjectssurya prakash pareek100% (1)