Das könnte Ihnen auch gefallen
- Quality Assurance ProgramDokument16 SeitenQuality Assurance ProgramMyca Omega Lacsamana100% (1)
- Introduction to Clinical Effectiveness and Audit in HealthcareVon EverandIntroduction to Clinical Effectiveness and Audit in HealthcareNoch keine Bewertungen
- Infection Control Program in The HospitalDokument14 SeitenInfection Control Program in The HospitalLorelie Asis100% (1)
- Line of Sight: How Improved Information, Transparency, and Accountability Would Promote the Adequate Resourcing of Health Facilities Across Papua New GuineaVon EverandLine of Sight: How Improved Information, Transparency, and Accountability Would Promote the Adequate Resourcing of Health Facilities Across Papua New GuineaNoch keine Bewertungen
- 9 6 Policy On Quality Assurance in Health Care ServicesDokument7 Seiten9 6 Policy On Quality Assurance in Health Care ServicesSujan AcharyaNoch keine Bewertungen
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsVon EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsNoch keine Bewertungen
- Homecare Guidance - 2019Dokument19 SeitenHomecare Guidance - 2019ahamedsahibNoch keine Bewertungen
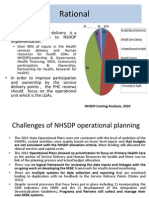
- Equity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiDokument34 SeitenEquity and Monitoring Progress of The NSHDP in Nigeria - The PHC Reviews by DR Eboreime EjemaiEjemai EboreimeNoch keine Bewertungen
- Healt Care Reform of PakistanDokument15 SeitenHealt Care Reform of Pakistanfarooq hayatNoch keine Bewertungen
- Impact Evaluation Study On The Bank Assistance in The Health and Population Sector in Sri LankaDokument24 SeitenImpact Evaluation Study On The Bank Assistance in The Health and Population Sector in Sri LankaIndependent Evaluation at Asian Development BankNoch keine Bewertungen
- Negros PIPHDokument64 SeitenNegros PIPHRose AnnNoch keine Bewertungen
- Clinical Governance in The UK NHSDokument4 SeitenClinical Governance in The UK NHSchiefsanjivNoch keine Bewertungen
- Health Sector Indicator Manual - Full Version - Final 4.12.2012Dokument235 SeitenHealth Sector Indicator Manual - Full Version - Final 4.12.2012stevekonahNoch keine Bewertungen
- Haliima DocumentDokument8 SeitenHaliima DocumentSacdiya MurzalNoch keine Bewertungen
- Helpdesk Report: Evidence Base For Local Block Grants in HealthDokument20 SeitenHelpdesk Report: Evidence Base For Local Block Grants in HealthCandra, MPHNoch keine Bewertungen
- Core Resilientsustainablesystemsforhealth Infonote enDokument35 SeitenCore Resilientsustainablesystemsforhealth Infonote enSponge BobNoch keine Bewertungen
- Clinical Care Quality Assurance Conference 2012Dokument28 SeitenClinical Care Quality Assurance Conference 2012El Min ForoNoch keine Bewertungen
- Philippine Health Care Delivery SystemDokument31 SeitenPhilippine Health Care Delivery SystemGOODWIN GALVANNoch keine Bewertungen
- Program For The Consultative Workshop Towards Quality Health Care Services in Khyber PakhtunkhwaDokument15 SeitenProgram For The Consultative Workshop Towards Quality Health Care Services in Khyber PakhtunkhwaADB Health Sector GroupNoch keine Bewertungen
- (2010) Group 15 Performance EvaluationDokument38 Seiten(2010) Group 15 Performance EvaluationSapna BansalNoch keine Bewertungen
- Clinical Audit Manual July, 2016Dokument21 SeitenClinical Audit Manual July, 2016Addishiwot seifuNoch keine Bewertungen
- MODULE 1: Healthcare System in KenyaDokument13 SeitenMODULE 1: Healthcare System in KenyaDrMohamed MansourNoch keine Bewertungen
- Pnadb 668Dokument16 SeitenPnadb 668Dracule MihawkNoch keine Bewertungen
- Draft Implementation Guideline: Health Service Extension ProgrammeDokument41 SeitenDraft Implementation Guideline: Health Service Extension ProgrammeWorkineh ChekolNoch keine Bewertungen
- Functional Clustering of DOH Units and Attached Agencies For Implementation of The Aquino Health Agenda To Achieve Universal Health CareDokument19 SeitenFunctional Clustering of DOH Units and Attached Agencies For Implementation of The Aquino Health Agenda To Achieve Universal Health CareAlbert DomingoNoch keine Bewertungen
- Clinic Supervisors Manual PDFDokument202 SeitenClinic Supervisors Manual PDFnawaflehNoch keine Bewertungen
- Process Quality - III - 2005 - 2010 - Outcome or Impact QualityDokument2 SeitenProcess Quality - III - 2005 - 2010 - Outcome or Impact QualityLuiciaNoch keine Bewertungen
- Process Quality - III - 2005 - 2010 - Outcome or Impact QualityDokument2 SeitenProcess Quality - III - 2005 - 2010 - Outcome or Impact QualityLuiciaNoch keine Bewertungen
- Combine Majpr TopicsDokument86 SeitenCombine Majpr TopicsDr. Pooja DubeyNoch keine Bewertungen
- Understanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiDokument34 SeitenUnderstanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiEjemai EboreimeNoch keine Bewertungen
- Ethiopian Health Care ReformDokument13 SeitenEthiopian Health Care ReformRobel areaNoch keine Bewertungen
- Indian Public Health Standard CHC Draft8march FinalDokument76 SeitenIndian Public Health Standard CHC Draft8march FinalSaqib NawazNoch keine Bewertungen
- Accreditation of Health Facilities Organizational Framework - IndiaDokument70 SeitenAccreditation of Health Facilities Organizational Framework - IndiaPaul PriyarajNoch keine Bewertungen
- Policy Memo - IDSR Ghana - Badu SarkodieDokument3 SeitenPolicy Memo - IDSR Ghana - Badu SarkodieJohnStephenJaneskiNoch keine Bewertungen
- Health Service Management at Lamjung District HospitalDokument102 SeitenHealth Service Management at Lamjung District HospitalShashanka PoudelNoch keine Bewertungen
- BegusaraiDokument102 SeitenBegusaraiAbhishek SharmaNoch keine Bewertungen
- Ministry of Health and Family WelfareDokument8 SeitenMinistry of Health and Family WelfareAakashMalhotraNoch keine Bewertungen
- KHFA 2018 19 Popular Version Report FinalDokument96 SeitenKHFA 2018 19 Popular Version Report FinalgramedincNoch keine Bewertungen
- Sanitation Problem Health SectorDokument44 SeitenSanitation Problem Health SectordeliapatrisaNoch keine Bewertungen
- SOP - HIV Care Patient Follow-Up ProgrammeDokument23 SeitenSOP - HIV Care Patient Follow-Up ProgrammeParwatiNoch keine Bewertungen
- Ghana E-Health120504121543Dokument80 SeitenGhana E-Health120504121543Issah Abdullai GombillaNoch keine Bewertungen
- CBRT PHC Report May09Dokument52 SeitenCBRT PHC Report May09Bryan tsepang NareNoch keine Bewertungen
- GAIHN Business Case Executive Summary FINALDokument38 SeitenGAIHN Business Case Executive Summary FINALsynergianzNoch keine Bewertungen
- Hospital Planning and Design-Unit 1Dokument25 SeitenHospital Planning and Design-Unit 1Timothy Suraj0% (1)
- Chapter 3Dokument23 SeitenChapter 3hgvfz4pcw4Noch keine Bewertungen
- 2020-0034 Revised Guidelines On The Implementation of CQI ProgramDokument13 Seiten2020-0034 Revised Guidelines On The Implementation of CQI ProgramBea MagbanuaNoch keine Bewertungen
- National Policy Quality and Safety PDFDokument11 SeitenNational Policy Quality and Safety PDFTharanga RNoch keine Bewertungen
- COVID 19 Report ArbaminchDokument4 SeitenCOVID 19 Report ArbaminchAmen Haleluya MisganaNoch keine Bewertungen
- Updates On The Implementation of Health Reforms and The Millennium Development GoalsDokument31 SeitenUpdates On The Implementation of Health Reforms and The Millennium Development GoalsSeriel TismoNoch keine Bewertungen
- Operational Guidelines For HWCDokument83 SeitenOperational Guidelines For HWCharleenNoch keine Bewertungen
- QA Operational Manual For RCHDokument135 SeitenQA Operational Manual For RCHJayanta Bhowmick0% (1)
- ncm-104: Community Health Nursing I: Jennifer J. Valero, Man-Rn Clinical InstructorDokument48 Seitenncm-104: Community Health Nursing I: Jennifer J. Valero, Man-Rn Clinical InstructorCorpus, Irene Zen P.100% (2)
- Project Work 2Dokument33 SeitenProject Work 2Job Akpelimtera NyaabaNoch keine Bewertungen
- ACCOUNTING PRACTICES OF HEALTHCARE INSTITUTIONS IN THE GHANAIAN PUBLIC SECTOR - A Case of 37 Military HospitalDokument59 SeitenACCOUNTING PRACTICES OF HEALTHCARE INSTITUTIONS IN THE GHANAIAN PUBLIC SECTOR - A Case of 37 Military HospitalAkwasi Adu Biggs II100% (1)
- Normes Ethique OoasDokument117 SeitenNormes Ethique OoasakowemagnificatNoch keine Bewertungen
- Health Sector Reform AgendaDokument2 SeitenHealth Sector Reform AgendaLhynne Riano Salando100% (1)
- Challenges & Achievements of NRHMDokument3 SeitenChallenges & Achievements of NRHMRenu R NairNoch keine Bewertungen
- 13 Sample BusinessDokument6 Seiten13 Sample Businessnimisha vermaNoch keine Bewertungen
- Health Referral System Manual - Central VisayasDokument103 SeitenHealth Referral System Manual - Central VisayasAlfred Russel Wallace50% (10)
- Emerging Management Practices in Teaching HospitalsDokument17 SeitenEmerging Management Practices in Teaching HospitalsSimon DzokotoNoch keine Bewertungen
- Ma Do Wo de DziDokument1 SeiteMa Do Wo de DziSimon DzokotoNoch keine Bewertungen
- Planning and Implementing RetreatsDokument9 SeitenPlanning and Implementing RetreatsSimon DzokotoNoch keine Bewertungen
- Why JCI For Laboratory AccreditationDokument2 SeitenWhy JCI For Laboratory AccreditationSimon DzokotoNoch keine Bewertungen
- HR Report For Handing OverDokument19 SeitenHR Report For Handing OverSimon DzokotoNoch keine Bewertungen
- Trauma Society of GhanaDokument5 SeitenTrauma Society of GhanaSimon DzokotoNoch keine Bewertungen
- Choice of ModelsDokument2 SeitenChoice of ModelsSimon DzokotoNoch keine Bewertungen
- Rational Use of Medicines & NHIS Tariff ImplementationDokument11 SeitenRational Use of Medicines & NHIS Tariff ImplementationSimon DzokotoNoch keine Bewertungen
- Unit Estates Determining Key Indicators For Nursing and Midwifery CouncilDokument2 SeitenUnit Estates Determining Key Indicators For Nursing and Midwifery CouncilSimon DzokotoNoch keine Bewertungen
- Development of A Multi Year Strategic Plan For Cape Coast Teaching HospitalDokument11 SeitenDevelopment of A Multi Year Strategic Plan For Cape Coast Teaching HospitalSimon DzokotoNoch keine Bewertungen
- MTN GHana Foundation Guidelines On Proposal SubmissionDokument1 SeiteMTN GHana Foundation Guidelines On Proposal SubmissionSimon Dzokoto100% (4)
- Programme For Mid Year ReviewDokument3 SeitenProgramme For Mid Year ReviewSimon DzokotoNoch keine Bewertungen
- Development of Business Plan For A HighDokument1 SeiteDevelopment of Business Plan For A HighSimon DzokotoNoch keine Bewertungen
- Constitutioin of The GEC Accra Presbytery Choirmasters' UnionDokument21 SeitenConstitutioin of The GEC Accra Presbytery Choirmasters' UnionSimon Dzokoto100% (1)
- RapporteurDokument11 SeitenRapporteurSimon DzokotoNoch keine Bewertungen
- AssessmentDokument24 SeitenAssessmentSimon DzokotoNoch keine Bewertungen
- PPP Sla Template-EnDokument18 SeitenPPP Sla Template-EnĐỗ Mai HươngNoch keine Bewertungen
- Un Pabnn 044791Dokument21 SeitenUn Pabnn 044791Simon DzokotoNoch keine Bewertungen
- Annex 1. Overview Timetable: Term 1Dokument2 SeitenAnnex 1. Overview Timetable: Term 1Simon DzokotoNoch keine Bewertungen
- Programme: Because Everyone CountsDokument3 SeitenProgramme: Because Everyone CountsSimon DzokotoNoch keine Bewertungen
- Professional Indicators - Other Wards 2012Dokument2 SeitenProfessional Indicators - Other Wards 2012Simon DzokotoNoch keine Bewertungen
- Professional Indicators - Maternity 2012Dokument6 SeitenProfessional Indicators - Maternity 2012Simon DzokotoNoch keine Bewertungen
- Medical Record Review FormDokument3 SeitenMedical Record Review FormSimon Dzokoto100% (1)
- Placenta AcretaDokument118 SeitenPlacenta AcretaPaco Vega WooNoch keine Bewertungen
- Application For Leave: Republic of The PhilippinesDokument2 SeitenApplication For Leave: Republic of The PhilippinesVaness Flor Cabug PuyatNoch keine Bewertungen
- Uterine RuptureDokument4 SeitenUterine RuptureTaloy MoralesNoch keine Bewertungen
- Aman Mbembela ProposalDokument37 SeitenAman Mbembela ProposalNyagawa GodkNoch keine Bewertungen
- Patient History FormDokument2 SeitenPatient History FormHelmiNoch keine Bewertungen
- Jurnal Kukerta Terintegrasi AbdimasDokument5 SeitenJurnal Kukerta Terintegrasi AbdimasholaNoch keine Bewertungen
- EmdrDokument33 SeitenEmdrShanker Iyer100% (1)
- Midwife 2Dokument65 SeitenMidwife 2jancyraniJNoch keine Bewertungen
- Doh NOTES-1Dokument196 SeitenDoh NOTES-1norabilbaoNoch keine Bewertungen
- Which Is The Primary Goal of Community Health NursingDokument20 SeitenWhich Is The Primary Goal of Community Health NursingKeepItSecretNoch keine Bewertungen
- Prophylactic AntibioticsDokument5 SeitenProphylactic AntibioticsponekNoch keine Bewertungen
- AOGD Bulletin December 2019Dokument68 SeitenAOGD Bulletin December 2019Abhilekh SrivastavaNoch keine Bewertungen
- CASE STUDY: Pre Labor Infant With Respiratory Distress SyndromeDokument4 SeitenCASE STUDY: Pre Labor Infant With Respiratory Distress SyndromeE.R.ONoch keine Bewertungen
- Case Analysis - Pregnant With AsthmaDokument1 SeiteCase Analysis - Pregnant With AsthmaJanine mae MacaraigNoch keine Bewertungen
- Etiologies and Risk Factors of Placental Abruption.402Dokument1 SeiteEtiologies and Risk Factors of Placental Abruption.402Sohaib AliNoch keine Bewertungen
- Cervical InsufficiencyDokument2 SeitenCervical InsufficiencyShe that BoyNoch keine Bewertungen
- 1 Inversion of UterusDokument44 Seiten1 Inversion of UterusSanthosh.S.UNoch keine Bewertungen
- MNCHNDokument45 SeitenMNCHNAnn Margareth Salazar-ManaloNoch keine Bewertungen
- Assess Knowledge and Practice Regarding Partograph Among Staff Nurses: Pre Experimental StudyDokument5 SeitenAssess Knowledge and Practice Regarding Partograph Among Staff Nurses: Pre Experimental StudyDiksha chaudharyNoch keine Bewertungen
- Stages of LaborDokument5 SeitenStages of Laborchrisanne09Noch keine Bewertungen
- Components of Consumer HealthDokument2 SeitenComponents of Consumer HealthRommiel Clanza100% (1)
- Skims Syllabus Staff NurseDokument9 SeitenSkims Syllabus Staff NurseWani Zahoor50% (2)
- Diet Pada Pasien Bedah Caesarea Section PDFDokument32 SeitenDiet Pada Pasien Bedah Caesarea Section PDFnovi rahmawatiNoch keine Bewertungen
- Case PresDokument26 SeitenCase PresRenz BaldonNoch keine Bewertungen
- Uterine and Vaginal Prolapse in EwesDokument6 SeitenUterine and Vaginal Prolapse in EwesfrankyNoch keine Bewertungen
- A Conceptual Guide To MRCP (Uk) Paces Exam.: Station 2, 4 and 5. SampleDokument29 SeitenA Conceptual Guide To MRCP (Uk) Paces Exam.: Station 2, 4 and 5. Samplesoe100% (1)
- Self-Medication and Safety Profile of Medicines Used Among Pregnant Women in A Tertiary Teaching Hospital in Jimma, Ethiopia: A Cross-Sectional StudyDokument15 SeitenSelf-Medication and Safety Profile of Medicines Used Among Pregnant Women in A Tertiary Teaching Hospital in Jimma, Ethiopia: A Cross-Sectional StudyahmedNoch keine Bewertungen
- Neonatal InfectionDokument19 SeitenNeonatal InfectionLekshmi ManuNoch keine Bewertungen
- NS 1 QUIZ 3 For PrintingDokument4 SeitenNS 1 QUIZ 3 For PrintingJe KirsteneNoch keine Bewertungen
- Almonte HistoryDokument3 SeitenAlmonte HistoryAngelo ErispeNoch keine Bewertungen
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicVon EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNoch keine Bewertungen
- Hero Found: The Greatest POW Escape of the Vietnam WarVon EverandHero Found: The Greatest POW Escape of the Vietnam WarBewertung: 4 von 5 Sternen4/5 (19)
- Sully: The Untold Story Behind the Miracle on the HudsonVon EverandSully: The Untold Story Behind the Miracle on the HudsonBewertung: 4 von 5 Sternen4/5 (103)
- The End of Craving: Recovering the Lost Wisdom of Eating WellVon EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellBewertung: 4.5 von 5 Sternen4.5/5 (82)
- The Future of Geography: How the Competition in Space Will Change Our WorldVon EverandThe Future of Geography: How the Competition in Space Will Change Our WorldBewertung: 4 von 5 Sternen4/5 (6)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- Mini Farming: Self-Sufficiency on 1/4 AcreVon EverandMini Farming: Self-Sufficiency on 1/4 AcreBewertung: 4 von 5 Sternen4/5 (76)
- The Fabric of Civilization: How Textiles Made the WorldVon EverandThe Fabric of Civilization: How Textiles Made the WorldBewertung: 4.5 von 5 Sternen4.5/5 (58)
- Dirt to Soil: One Family’s Journey into Regenerative AgricultureVon EverandDirt to Soil: One Family’s Journey into Regenerative AgricultureBewertung: 5 von 5 Sternen5/5 (125)
- When the Heavens Went on Sale: The Misfits and Geniuses Racing to Put Space Within ReachVon EverandWhen the Heavens Went on Sale: The Misfits and Geniuses Racing to Put Space Within ReachBewertung: 3.5 von 5 Sternen3.5/5 (6)
- Transformed: Moving to the Product Operating ModelVon EverandTransformed: Moving to the Product Operating ModelBewertung: 4 von 5 Sternen4/5 (1)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineVon EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNoch keine Bewertungen
- System Error: Where Big Tech Went Wrong and How We Can RebootVon EverandSystem Error: Where Big Tech Went Wrong and How We Can RebootNoch keine Bewertungen
- The Beekeeper's Lament: How One Man and Half a Billion Honey Bees Help Feed AmericaVon EverandThe Beekeeper's Lament: How One Man and Half a Billion Honey Bees Help Feed AmericaNoch keine Bewertungen
- Fire on the Horizon: The Untold Story of the Gulf Oil DisasterVon EverandFire on the Horizon: The Untold Story of the Gulf Oil DisasterNoch keine Bewertungen
- Highest Duty: My Search for What Really MattersVon EverandHighest Duty: My Search for What Really MattersNoch keine Bewertungen
- The Intel Trinity: How Robert Noyce, Gordon Moore, and Andy Grove Built the World's Most Important CompanyVon EverandThe Intel Trinity: How Robert Noyce, Gordon Moore, and Andy Grove Built the World's Most Important CompanyNoch keine Bewertungen
- Faster: How a Jewish Driver, an American Heiress, and a Legendary Car Beat Hitler's BestVon EverandFaster: How a Jewish Driver, an American Heiress, and a Legendary Car Beat Hitler's BestBewertung: 4 von 5 Sternen4/5 (28)
- Permaculture for the Rest of Us: Abundant Living on Less than an AcreVon EverandPermaculture for the Rest of Us: Abundant Living on Less than an AcreBewertung: 4.5 von 5 Sternen4.5/5 (33)
- Restoration Agriculture: Real-World Permaculture for FarmersVon EverandRestoration Agriculture: Real-World Permaculture for FarmersBewertung: 4.5 von 5 Sternen4.5/5 (86)
- Process Plant Equipment: Operation, Control, and ReliabilityVon EverandProcess Plant Equipment: Operation, Control, and ReliabilityBewertung: 5 von 5 Sternen5/5 (1)
- Reality+: Virtual Worlds and the Problems of PhilosophyVon EverandReality+: Virtual Worlds and the Problems of PhilosophyBewertung: 4 von 5 Sternen4/5 (24)
- ChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindVon EverandChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindNoch keine Bewertungen
- Pale Blue Dot: A Vision of the Human Future in SpaceVon EverandPale Blue Dot: A Vision of the Human Future in SpaceBewertung: 4.5 von 5 Sternen4.5/5 (588)
- The Technology Trap: Capital, Labor, and Power in the Age of AutomationVon EverandThe Technology Trap: Capital, Labor, and Power in the Age of AutomationBewertung: 4.5 von 5 Sternen4.5/5 (46)