Viewpoint
Child undernutrition, tropical enteropathy, toilets, and handwashing
Jean H Humphrey
Lancet 2009; 374: 103235 Center for Human Nutrition, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA, and ZVITAMBO project, Harare, Zimbabwe (J H Humphrey ScD) Correspondence to: Dr Jean H Humphrey, Johns Hopkins Bloomberg School of Public Health, Center for Human Nutrition, 615 N Wolfe Street, Baltimore, MD 21205, USA jhumphrey@zvitambo.co.zw
Of the 555 million preschool children in developing countries, 32% are stunted and 20% are underweight.1 Child underweight or stunting causes about 20% of all mortality of children younger than 5 years of age and leads to long-term cognitive decits, poorer performance in school and fewer years of completed schooling, and lower adult economic productivity.2 Child underweight state or stunting mainly develops during the rst 2 years of life, when mean weight-for-age and length-for-age Z scores of children in Africa and Asia drop to about 20, with little or no recovery thereafter.3 Under the plausible assumption that children grow poorly because they do not eat enough of the right foods, research eorts have focused on identifying dietary solutions. Numerous studies have tested many nutrient-dense foods and supplements, nutrition education interventions, and infant feeding behaviouralchange strategies. A recent review4 of 38 of these studies showed that children receiving one of these dietary interventions gained up to 760 g more weight (00076 weight-for-age Z score) and grew up to 17 cm taller (00064 length-for-age Z score) than control children by 12 to 24 months. However, none of these interventions achieved normal growth: the growth eect of even the most successful of these studies (~ +07 Z) is equivalent to about a third of the average decit of Asian and African children (~ 20 Z). Diarrhoea has also been implicated as a cause of poor growth. In a pooled analysis of nine studies with diarrhoea and growth data for 1393 children,5 the probability of stunting at 24 months of age increased by 25% per episode of diarrhoea, and 25% of all stunting in 24-month-old children was attributable to having ve or more episodes of diarrhoea in the rst 2 years of life. However, other authors have contended that the eect of diarrhoea on permanent stunting is small because growth velocity can be faster than average for age between illness episodes resulting in catch-up growth.6 Hence, the relative contribution of diarrhoea to undernutrition and, consequently, the potential eect that diarrhoea control programmes (ie, sanitation and hygiene interventions) could have on growth are still unresolved. The Lancet Maternal and Child Undernutrition Series estimated that sanitation and hygiene interventions implemented with 99% coverage would reduce diarrhoea incidence by 30%, which would in turn decrease the prevalence of stunting by only 24%.7 This report suggests: that a key cause of child undernutrition is a subclinical disorder of the small intestine known as tropical enteropathy, which is characterised by villous atrophy, crypt hyperplasia,
increased permeability, inammatory cell inltrate, and modest malabsorption;8 that tropical enteropathy is caused by faecal bacteria ingested in large quantities by young children living in conditions of poor sanitation and hygiene; that provision of toilets and promotion of handwashing after faecal contact could reduce or prevent tropical enteropathy and its adverse eects on growth; and that the primary causal pathway from poor sanitation and hygiene to undernutrition is tropical enteropathy and not diarrhoea. If this is true, the Lancet Maternal and Child Undernutrition Series7 might have substantially underestimated the contribution of sanitation and hygiene to growth because the eect was modelled entirely through diarrhoea. Importantly, because of mortality, and cognitive and economic consequences of child undernutrition, sanitation and hygiene interventions might have been undervalued because they have been mainly appraised for their eect on diarrhoea. Conrmation of these hypotheses might provide evidence to accelerate provision of toilets to the 26 billion people (40% of the worlds population) who currently lack them, hasten progress towards the Millennium Development Goal to halve this number by 2015, and ultimately yield improvements in child growth, health, and survival. Several studies done mostly in the 1960s in Asia, Africa, and Central America showed that almost all apparently healthy adults and children in developing countries worldwide had morphological changes or functional signs of tropical enteropathy.8 Although the cause of tropical enteropathy has not been clearly elucidated, most of these investigators suggested that tropical enteropathy results from exposure to poor environmental sanitation. Further evidence for an environmental cause comes from studies of asymptomatic American soldiers in Vietnam and Peace Corps volunteers in Pakistan who got tropical enteropathy after a few months of residence in these settings and recovered soon after returning to the USA.8 Similar to other inammatory bowel diseases, tropical enteropathy results from unrestrained enteric T-cell activation.9 However, unlike diseases caused by abnormal hyper-reactivity to a normal exposure (eg, in coeliac disease, enteric T cells are phenotypically hyper-reactive to gluten10), tropical enteropathy probably develops when normal T cells are hyperstimulated by abnormally high concentrations of ingested faecal bacteria in the small-intestinal lumen.11 Over the past 20 years, investigators at the MRC Dunn Nutritional Laboratory (Cambridge, UK, and Keneba, The Gambia) have studied growth in Gambian children. Dietary inadequacy and diarrhoea were not associated
www.thelancet.com Vol 374 September 19, 2009
1032
Viewpoint
No toilet
Faecal contamination of domestic environment
Faecal contamination of infant hands
Faecal ingestion by infants and young children
Increased pathogenic bacteria ingestion
No handwashing after faecal contact
Faecal contamination of breast, infant food, drinking water, utensils, toys
High bacterial ingestion overwhelms gastric barrier resulting in high bacteria concentration in the small-intestinal lumen
Intermittent diarrhoea
Faecal contamination of child caretakers hands
Enteric T-cell stimulation
Tropical enteropathy Chronic villus atrophy, crypt hyperplasia, inammatory cell inltrate
Anorexia
Reduced small-intestinal surface area
Increased intestinal permeability
Reduced nutrient absorption
Microbial translocation
Repartitioning of exogenous and endogenous nutrients away from growth for: increased synthesis of antibodies (including EndoCAb), acute-phase proteins, cytokines, and increased glucose oxidation to fuel high metabolic rate
Multiple socio-economic, climatic, political, and behavioural factors
Reduced nutrient absorption
Child undernutrition
Inadequate diet
Increased child mortality Reduced cognitive development and adult economic productivity
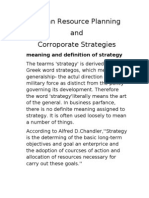
Figure: Model of the mechanisms from poor sanitation and hygiene to tropical enteropathy, child undernutrition, and child development and survival Thick lines indicate primary pathways and thin lines secondary pathways, as hypothesised in this report.
with growth failure, but the lactulose to mannitol urinary excretion ratioan indicator of intestinal permeability explained 39% of ponderal and 43% of linear growth.12 Moreover, gut hyperpermeability was a chronic condition: these children had diarrhoea on 73% of days between birth and 2 years of life, but had lactulose to mannitol urinary excretion ratios associated with growth suppression on 76% of days during this period. In a subsequent study,13 the same investigators also measured plasma concentrations of total IgG and IgGendotoxin-core antibody (EndoCAb). Endotoxin is a component of gram-negative bacterial cell walls probably derived from faecal contamination. A permeable gut allows endotoxin translocation into the body, where it stimulates an immune response that stimulates production of EndoCAb. At 2 months of age, the weightfor-age Z score, height-for-age Z score, lactulose to mannitol ratio, and plasma IgG and EndoCAb concentrations were similar to those in normal infants in
www.thelancet.com Vol 374 September 19, 2009
the UK. However, by 15 months of age, mean height-forage Z score fell from 06 to 18, mean weight-for-age Z score fell from 04 to 24, the lactulose to mannitol ratio almost tripled (in normal infants in the UK, this ratio declined during this period), and mean IgG and EndoCAb concentrations were 2-fold and 5-fold higher than normal, respectively. The lactulose to mannitol ratio and IgG and EndoCAb concentrations were correlated with each other and all were negatively correlated with linear and ponderal growth. Using semipartial regression analysis methods, the combined eects of IgG and EndoCAb concentrations explained 51% of linear growth, which increased to 56% when the lactulose to mannitol ratio was also included. Solomons and colleagues tell a similar story from animal husbandry.14 In controlled studies, chicks raised amidst faeces, dust, and dander but fed antibiotics grew better than chicks living in similar conditions but not fed antibiotics, and grew as well as chicks raised in
1033
Viewpoint
steam-cleaned cages for whom antibiotics had no growth eect.15 The poor growth of dirty chicks not fed antibiotics was accompanied by high plasma concentrations of interleukin 1, a major mediator of the immune response, which was not observed in dirty chicks fed antibiotics or in clean chicks. On this basis, antibiotics (termed growth permitters in this context) have been used for decades on poultry farms to maximise meat yield. Therefore, when confronted by incessant microbial challenge, both the Gambian infants and chicks studied entered a near-continuous state of growth-suppressing immune response: dietary nutrients were repartitioned away from anabolism in favour of glucose oxidation and synthesis of acute-phase proteins and other immune mediators.14 The gure shows a model of these pathways. Children living in poor sanitary conditions ingest high concentrations of faecal bacteria, which colonise the small intestine and induce tropical enteropathy through a T-cell-mediated process. The hyperpermeable gut facilitates translocation of microbes, which trigger the metabolic changes of the immune response. Growth falters when these changes coincide with reduced nutrient absorption by atrophied villi, marginal dietary intake, and the high growth demands of the rst 2 years of life. How can children be protected from faeces? Safe disposal of stools (ie, toilets) and handwashing with soap after faecal contact are the primary barriers to faecal-oral transmission because they prevent faeces from entering the domestic environment. Many randomised trials of handwashing16 have shown substantial reductions in diarrhoea, although none included the eect of these interventions on tropical enteropathy or child growth. Surprisingly, there are no published randomised trials of toilet provision on child growth or even diarrhoea. Almost all existing evidence that sanitation benets human health comes from cross-sectional, prospective cohort, case-control, and non-randomised intervention studies. Thus, all have methodological issues, including potential confounding by socioeconomic status, lack of adequate control in beforeafter programme assessments, and inadequate statistical power when a single control community is compared with a single intervention community.17 Nonetheless, many of these studies have documented benets on child growth.18 Indeed, in an analysis of demographic and health survey data from eight countries, Esrey19 estimated that improvements in sanitation were associated with length-for-age Z score increments of 006062 in children living in rural areas and 026065 in children living in urban areas, which are similar to the growth eects of dietary interventions reviewed earlier in this report4 (ie, 000064). Moreover, from a mean length-for-age Z score (SD) of 169 (145) in rural children and 119 (145) in urban children, these increments correspond to 437% and 2046% decreases
1034
in stunting prevalence in rural and urban children, respectively, suggesting a considerably greater eect than the 24% decrease previously estimated in the Lancet Series.7 Undoubtedly, the complex problem of child undernutrition will not be solved with toilets and handwashing alone. Interventions focused on gut microbial populations20 and improved drinking water quality21 might be important, together with continued eorts to improve infant diets. However, I hypothesise that prevention of tropical enteropathy, which aicts almost all children in the developing world, will be crucial to normalise child growth, and that this will not be possible without provision of toilets. Randomised controlled trials of toilet provision and handwashing promotion that include tropical enteropathy and child growth as outcomes will give valuable evidence for this premise, and might oer a solution to the intractable problem of child undernutrition.
Conicts of interest I declare that I have no conicts of interest. Acknowledgments I thank Robert Ntozini for statistical support; Prof Rebecca Stoltzfus and Prof Robert Black for helpful comments on earlier versions of this paper; and UK Department for International Development and US National Institutes of Child Health and Human Development (grant number: 1R01HD060338-01) for nancial support. References 1 Black RE, Allen LH, Bhutta ZA, et al. Maternal and undernutrition: global and regional exposures and health consequences. Lancet 2008; 371: 24360. 2 Victora CG, Adair L, Fall C, et al. Maternal and child undernutrition 2: Maternal and child undernutrition: consequences for adult health and human capital. Lancet 2008; 371: 34057. 3 Shrimpton R, Victora CG, De Onis M, Lima RC, Blossner M, Clugston G. Worldwide timing of growth faltering: implications for nutritional interventions. Pediatrics 2001; 107: 17. 4 Dewey KG, Adu-Afarwuah S. Systematic review of the ecacy and eectiveness of complementary feeding interventions in developing countries. In: Maternal and Child Nutrition. Blackwell Publishing Ltd: Program in International and Community Nutrition, University of California, Davis, CA, USA, 2008; pp 2485. 5 Checkley W, Buckley G, Gilman RH, et al, The Childhood Malnutrition and Infection Network. Multi-country analysis of the eects of diarrhoea on childhood stunting. Int J Epidemiol 2008; 37: 81630. 6 Briend A. Is diarrhoea a major cause of malnutrition among the under-ves in developing countries? A review of available evidence. Eur J Clin Nutr 1990; 44: 61128. 7 Bhutta ZA, Ahmed T, Black RE, et al. Maternal and child undernutrition 3: What works? Interventions for maternal and child undernutrition and survival. Lancet 2008; 371: 41740. 8 Haghighi P, Wolf PL. Tropical sprue and subclinical enteropathy: a vision for the nineties. Crit Rev Clin Lab Sci 1997; 34: 31341. 9 Veitch AM, Kelly P, Zulu IS, Segal I, Farthing MJG. Tropical enteropathy: a T-cell-mediated crypt hyperplastic enteropathy. Eur J Gastroenterol Hepatol 2001; 13: 117581. 10 Halstensen TS, Brandtzaeg P. Activated T lymphcytes in the celiac lesion: non-proliferative activation (CD25) of CD+ a/b cells in the lamina propria but proliferation (Ki-67) of a/b and gd cells in the epithelium. Eur J Immunol 1993; 23: 50510. 11 Fagundes Neto U, Martins MC, Lima FL, Patricio FR, Toledo MR. Asymptomatic environmental enteropathy among slum-dwelling infants. J Am Coll Nutr 1994; 13: 5156. 12 Lunn PG, Northrop-Clewes CA, Downes RM. Intestinal permeability, mucosal injury, and growth faltering in Gambian infants. Lancet 1991; 338: 90710.
www.thelancet.com Vol 374 September 19, 2009
Viewpoint
13
14
15
16
Campbell DI, Elia M, Lunn PG. Growth faltering in rural Gambian infants is associated with impaired small intestinal barrier function, leading to endotoxemia and systemic inammation. J Nutr 2003; 133: 133238. Solomons NW, Mazariegos M, Brown KH, Klasing K. The underprivileged, developing country child:environmental contamination and growth failure revisited. Nutr Rev 1993; 51: 32732. Roura E, Homedes J, Klasing KC. Prevention of immunologic stress contributes to the growth-permitting ability of dietary antibiotics in chicks. J Nutr 1992; 122: 238390. Curtis V, Cairncross S. Eect of washing hands with soap on diarrhoea risk in the community: a systematic review. Lancet Infect Dis 2003; 3: 27581.
17
18
19 20
21
Blum B, Feachem RG. Measuring the impact of water supply and sanitation investments on diarrhoeal diseases: problems of methodology. Int J Epidemiol 1983; 12: 35765. Checkley W, Gilman RH, Black RE, et al. Eect of water and sanitation on childhood health in a poor Peruvian peri-urban community. Lancet 2004; 363: 11218. Esrey SA. Water, waste, and well-being: a multicountry study. Am J Epidemiol 1996; 143: 60823. Palmer C, Bik EM, DiGiulio DB, Relman DA, Brown PO. Development of the human infant intestinal microbiota. PLoS Med 2007; 5: e177. Clasen T, Schmidt W-P, Rabie T, Roberts I, Cairncross S. Interventions to improve water quality for preventing diarrhoea: systematic review and meta-analysis.BMJ 2007; 334: 782.
www.thelancet.com Vol 374 September 19, 2009
1035
Das könnte Ihnen auch gefallen
- Pojok Kang Hebring 5 April 2013Dokument1 SeitePojok Kang Hebring 5 April 2013STBM IndonesiaNoch keine Bewertungen
- Pojok Kang Hebring - 10 April 2013Dokument1 SeitePojok Kang Hebring - 10 April 2013STBM IndonesiaNoch keine Bewertungen
- Progress On Drinking-Water and Sanitation Special Focus On SanitationDokument58 SeitenProgress On Drinking-Water and Sanitation Special Focus On SanitationSTBM IndonesiaNoch keine Bewertungen
- The CLTS Story in IndonesiaDokument26 SeitenThe CLTS Story in IndonesiaSTBM IndonesiaNoch keine Bewertungen
- Final Report Sanitation Training and Capacity StudyDokument128 SeitenFinal Report Sanitation Training and Capacity StudySTBM Indonesia100% (1)
- A Simple Index To Measure Hygiene BehavioursDokument9 SeitenA Simple Index To Measure Hygiene BehavioursSTBM IndonesiaNoch keine Bewertungen
- Knowledge and Information Management in Water and Sanitation Sector A Hard Nut To CrackDokument66 SeitenKnowledge and Information Management in Water and Sanitation Sector A Hard Nut To CrackSTBM IndonesiaNoch keine Bewertungen
- Promoting Good Hygiene Practices: Key Elements and Practical LessonsDokument12 SeitenPromoting Good Hygiene Practices: Key Elements and Practical LessonsSTBM IndonesiaNoch keine Bewertungen
- Marketing Safe WaterDokument120 SeitenMarketing Safe WaterSTBM IndonesiaNoch keine Bewertungen
- Enabling Environment Assessment For Scaling Up Sanitation ProgramsDokument78 SeitenEnabling Environment Assessment For Scaling Up Sanitation ProgramsSTBM IndonesiaNoch keine Bewertungen
- The Hygiene Improvement Framework A Comprehensive Approach For Preventing Childhood DiarrheaDokument37 SeitenThe Hygiene Improvement Framework A Comprehensive Approach For Preventing Childhood DiarrheaSTBM Indonesia100% (1)
- Formative Research Report Hygiene Health IndonesiaDokument119 SeitenFormative Research Report Hygiene Health IndonesiaSTBM IndonesiaNoch keine Bewertungen
- Combating Waterborne Disease at The Household LevelDokument36 SeitenCombating Waterborne Disease at The Household LevelSTBM IndonesiaNoch keine Bewertungen
- Handwashing HandbookDokument80 SeitenHandwashing Handbookshivani3008Noch keine Bewertungen
- Enewsletter Sanitasi Total Berbasis Masyarakat STBM February 2012Dokument3 SeitenEnewsletter Sanitasi Total Berbasis Masyarakat STBM February 2012STBM IndonesiaNoch keine Bewertungen
- Handwashing For Preventing DiarrhoeaDokument44 SeitenHandwashing For Preventing DiarrhoeaSTBM IndonesiaNoch keine Bewertungen
- Building The Capacity of Local Government To Scale Up Community-Led Total Sanitation and Sanitation MarketingDokument72 SeitenBuilding The Capacity of Local Government To Scale Up Community-Led Total Sanitation and Sanitation MarketingSTBM IndonesiaNoch keine Bewertungen
- WHO Facts Figures 2005Dokument2 SeitenWHO Facts Figures 2005STBM IndonesiaNoch keine Bewertungen
- Facts and Figures About HandwashingDokument3 SeitenFacts and Figures About HandwashingSTBM Indonesia100% (1)
- Accelerating The Change: Selecting Best Practices To Promote Total Sanitation and Sanitation Marketing in East JavaDokument32 SeitenAccelerating The Change: Selecting Best Practices To Promote Total Sanitation and Sanitation Marketing in East JavaSTBM IndonesiaNoch keine Bewertungen
- Use of Ash and Mud For Handwashing in Low Income CommunitiesDokument40 SeitenUse of Ash and Mud For Handwashing in Low Income CommunitiesSTBM IndonesiaNoch keine Bewertungen
- Introducing SaniFOAM A Framework To Analyze Behaviors To Design Effective Sanitation ProgramsDokument28 SeitenIntroducing SaniFOAM A Framework To Analyze Behaviors To Design Effective Sanitation ProgramsSTBM IndonesiaNoch keine Bewertungen
- Raising Clean Hands 2010 - Advancing Learning, Health and Participation Through WASH in SchoolsDokument24 SeitenRaising Clean Hands 2010 - Advancing Learning, Health and Participation Through WASH in SchoolsUNICEF100% (3)
- Learning at ScaleDokument22 SeitenLearning at ScaleSTBM IndonesiaNoch keine Bewertungen
- Indonesia Sanitation Market Assessment 2010Dokument117 SeitenIndonesia Sanitation Market Assessment 2010STBM IndonesiaNoch keine Bewertungen
- Practical Guidance For Measuring Handwashing BehaviorDokument24 SeitenPractical Guidance For Measuring Handwashing BehaviorSTBM IndonesiaNoch keine Bewertungen
- Social Factor Impacting Use of Ecosan in Rural IndonesiaDokument4 SeitenSocial Factor Impacting Use of Ecosan in Rural IndonesiaSTBM IndonesiaNoch keine Bewertungen
- Why Is Handwashing ImportantDokument18 SeitenWhy Is Handwashing ImportantSTBM Indonesia100% (1)
- Health and Hygiene Promotion Best Practices and Lessons LearnedDokument56 SeitenHealth and Hygiene Promotion Best Practices and Lessons LearnedSTBM IndonesiaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Speeduino Manual-7Dokument16 SeitenSpeeduino Manual-7Makson VieiraNoch keine Bewertungen
- Human Resource Planning and Corroporate Strategies: Meaning and Definition of StrategyDokument19 SeitenHuman Resource Planning and Corroporate Strategies: Meaning and Definition of StrategyRashmi KhublaniNoch keine Bewertungen
- Sbi Home Loan InfoDokument4 SeitenSbi Home Loan InfoBhargavaSharmaNoch keine Bewertungen
- WBLFFDokument10 SeitenWBLFFMohd IzatNoch keine Bewertungen
- BICs Policy 2021 - FinalDokument8 SeitenBICs Policy 2021 - FinalIrfan U ShahNoch keine Bewertungen
- 2.1-Islamic Law of Contract and SalesDokument39 Seiten2.1-Islamic Law of Contract and SalesAllauddinagha100% (1)
- PCM320 IDM320 NIM220 PMM310 Base Release Notes 1210Dokument48 SeitenPCM320 IDM320 NIM220 PMM310 Base Release Notes 1210Eduardo Lecaros CabelloNoch keine Bewertungen
- 04 Vendor Registration TrainingDokument16 Seiten04 Vendor Registration TrainingAhmad Ramin AbasyNoch keine Bewertungen
- Gas Turbine MaintenanceDokument146 SeitenGas Turbine MaintenanceMamoun1969100% (8)
- European Management Journal: Pawel Korzynski, Grzegorz Mazurek, Michael HaenleinDokument9 SeitenEuropean Management Journal: Pawel Korzynski, Grzegorz Mazurek, Michael HaenleinkharismaNoch keine Bewertungen
- Watson Studio - IBM CloudDokument2 SeitenWatson Studio - IBM CloudPurvaNoch keine Bewertungen
- Underground Water Tanks Cleaning ScopeDokument2 SeitenUnderground Water Tanks Cleaning ScopeOsama AhmedNoch keine Bewertungen
- Cambridge Ext2 Ch1 Complex Numbers IWEBDokument62 SeitenCambridge Ext2 Ch1 Complex Numbers IWEBchenNoch keine Bewertungen
- Introduction To Computer Graphics: Version 1.3, August 2021Dokument456 SeitenIntroduction To Computer Graphics: Version 1.3, August 2021Sharan K.KNoch keine Bewertungen
- Business-Process Integration: Supply-Chain Management 2.0 (SCM 2.0)Dokument8 SeitenBusiness-Process Integration: Supply-Chain Management 2.0 (SCM 2.0)nidayousafzaiNoch keine Bewertungen
- Noor Hafifi Bin Jalal: Operating Code 1: Demand ForecastDokument47 SeitenNoor Hafifi Bin Jalal: Operating Code 1: Demand ForecastGopalakrishnan SekharanNoch keine Bewertungen
- Boosting BARMM Infrastructure for Socio-Economic GrowthDokument46 SeitenBoosting BARMM Infrastructure for Socio-Economic GrowthEduardo LongakitNoch keine Bewertungen
- Komatsu PC01-1 (JPN) 14001-Up Shop ManualDokument217 SeitenKomatsu PC01-1 (JPN) 14001-Up Shop Manualhaimay118100% (2)
- PTM Kel 4 (English)Dokument10 SeitenPTM Kel 4 (English)A'an Al FikriNoch keine Bewertungen
- LAB-Histopath Midterms 01Dokument5 SeitenLAB-Histopath Midterms 01Jashmine May TadinaNoch keine Bewertungen
- 150 C++ BitsDokument55 Seiten150 C++ BitsRavi Varma D V SNoch keine Bewertungen
- Community Health Nursing Family Nursing AssessmentDokument2 SeitenCommunity Health Nursing Family Nursing AssessmentRy LlanesNoch keine Bewertungen
- Ashok LeylandDokument4 SeitenAshok Leylandsodhiseema100% (1)
- Mémoire ENSMDokument97 SeitenMémoire ENSMAntoine Laurent100% (1)
- Martina: Available Colors For This VersionDokument2 SeitenMartina: Available Colors For This VersionUmeshNoch keine Bewertungen
- Essential Components of an Effective Road Drainage SystemDokument11 SeitenEssential Components of an Effective Road Drainage SystemRaisanAlcebarNoch keine Bewertungen
- Tax Invoice: New No 30, Old No 24 Bhagirathi Ammal ST, T Nagar, Chennai 600017 CIN: U74900TN2011PTC083121 State Code: 33Dokument1 SeiteTax Invoice: New No 30, Old No 24 Bhagirathi Ammal ST, T Nagar, Chennai 600017 CIN: U74900TN2011PTC083121 State Code: 33golu84Noch keine Bewertungen
- Image Authentication ENFSIDokument43 SeitenImage Authentication ENFSIIolanda OprisanNoch keine Bewertungen
- Global POVEQ NGADokument2 SeitenGlobal POVEQ NGABonifaceNoch keine Bewertungen
- Grand Central Terminal Mep Handbook 180323Dokument84 SeitenGrand Central Terminal Mep Handbook 180323Pete A100% (1)