Das könnte Ihnen auch gefallen
- Racism and Psychiatry: Contemporary Issues and InterventionsVon EverandRacism and Psychiatry: Contemporary Issues and InterventionsMorgan M. MedlockNoch keine Bewertungen
- Psychiatric Diagnosis: Challenges and ProspectsVon EverandPsychiatric Diagnosis: Challenges and ProspectsIhsan M. SalloumBewertung: 5 von 5 Sternen5/5 (1)
- Obsessive-Compulsive Disorder (OCD) Screening ToolDokument2 SeitenObsessive-Compulsive Disorder (OCD) Screening ToolManiya Dianne ReyesNoch keine Bewertungen
- Social Functioning QuestionnaireDokument3 SeitenSocial Functioning QuestionnaireMayang SelektaNoch keine Bewertungen
- The Psychiatric Assessment NotebookDokument4 SeitenThe Psychiatric Assessment NotebookSean Goddard NPNoch keine Bewertungen
- Conners2011 PDFDokument297 SeitenConners2011 PDFCristinaNoch keine Bewertungen
- No Evidence of DependenceDokument2 SeitenNo Evidence of Dependencemago1961Noch keine Bewertungen
- Guidline Threatment For of Alcohol Use DisorderDokument226 SeitenGuidline Threatment For of Alcohol Use Disorderafifberlian100% (1)
- The Clinical Assessment Interview For Negative SymDokument9 SeitenThe Clinical Assessment Interview For Negative SymJohanes DavidNoch keine Bewertungen
- Psychiatric Interview 2020 For Students (Clerking Pages)Dokument12 SeitenPsychiatric Interview 2020 For Students (Clerking Pages)jeff wingerNoch keine Bewertungen
- Calgary Depression Scale For Schizophrenia (CDSS)Dokument1 SeiteCalgary Depression Scale For Schizophrenia (CDSS)Edward Arthur IskandarNoch keine Bewertungen
- AsfdafsdDokument125 SeitenAsfdafsdfrankmalcovNoch keine Bewertungen
- Y Bocs Information SampleDokument2 SeitenY Bocs Information SampledevNoch keine Bewertungen
- Ayahuasca Pharmacology, Neuroscience and Therapeutic PotentialDokument13 SeitenAyahuasca Pharmacology, Neuroscience and Therapeutic PotentialSam JyotishiNoch keine Bewertungen
- Therapy Note 05-17-10Dokument1 SeiteTherapy Note 05-17-10Errata BNoch keine Bewertungen
- BprsDokument7 SeitenBprsamyljf100% (1)
- Schizoaffective Disorder in The DSM 5 PDFDokument5 SeitenSchizoaffective Disorder in The DSM 5 PDFpipiitopandabamboo247Noch keine Bewertungen
- Qids - SR: InstructionsDokument4 SeitenQids - SR: InstructionsPaul Benavidez100% (1)
- 2021-Editorial - Defining The Clinical Boundary of Disruptive Mood Dysregulation Disorder Symptoms in YouthDokument3 Seiten2021-Editorial - Defining The Clinical Boundary of Disruptive Mood Dysregulation Disorder Symptoms in YouthCaio MayrinkNoch keine Bewertungen
- Understanding DelusionsDokument17 SeitenUnderstanding DelusionsAnonymous 0ZZTYomaq100% (1)
- Ncmhce Sample Case StudiesDokument6 SeitenNcmhce Sample Case Studies002019ryNoch keine Bewertungen
- Quiz: Are You Ready To Be An Entrepreneur?: Yes NoDokument5 SeitenQuiz: Are You Ready To Be An Entrepreneur?: Yes NoAbhishek MohiteNoch keine Bewertungen
- Prescription Privileges For Psychologists PDFDokument16 SeitenPrescription Privileges For Psychologists PDFMarianaMoralesNoch keine Bewertungen
- Modified Sad Persons ScaleDokument1 SeiteModified Sad Persons ScaleFatin NabihahNoch keine Bewertungen
- Case Note Excellent2 AnnotatedDokument8 SeitenCase Note Excellent2 AnnotatedShubham Jain Modi100% (1)
- Triage ToolkitDokument8 SeitenTriage ToolkitZunni HermawatiNoch keine Bewertungen
- Manual 3Dokument89 SeitenManual 3Gio AlvarezNoch keine Bewertungen
- Disruptive Mood Dysregulation Disorder: Florian Daniel Zepf, Caroline Sarah Biskup, Martin Holtmann, & Kevin RunionsDokument17 SeitenDisruptive Mood Dysregulation Disorder: Florian Daniel Zepf, Caroline Sarah Biskup, Martin Holtmann, & Kevin RunionsPtrc Lbr LpNoch keine Bewertungen
- Adhd - Asrs .ScreenDokument4 SeitenAdhd - Asrs .ScreenKenth GenobisNoch keine Bewertungen
- Mental Health TipsDokument10 SeitenMental Health Tipsnicki scheffler100% (2)
- Scales For BIpolar DisorderDokument14 SeitenScales For BIpolar DisorderDivia RainaNoch keine Bewertungen
- PBL 3Dokument7 SeitenPBL 3UzmaNoch keine Bewertungen
- DWP Full Workbook PDFDokument115 SeitenDWP Full Workbook PDFBran KNoch keine Bewertungen
- Clinical Psychological Science 2016 Beck 2167702616628523Dokument24 SeitenClinical Psychological Science 2016 Beck 2167702616628523memo leyNoch keine Bewertungen
- Disorders RushedDokument40 SeitenDisorders Rushedapi-391411195Noch keine Bewertungen
- Aaseesment Scale For Cog RehabDokument9 SeitenAaseesment Scale For Cog Rehabmohitnet1327Noch keine Bewertungen
- Depression and Anxiety Essentials: Jessica L. Langenhan, MDDokument135 SeitenDepression and Anxiety Essentials: Jessica L. Langenhan, MDCoding NinjaNoch keine Bewertungen
- Catatonia PDFDokument9 SeitenCatatonia PDFDanilo RibeiroNoch keine Bewertungen
- .Suicidal Behaviors PDFDokument184 Seiten.Suicidal Behaviors PDFedidrimaNoch keine Bewertungen
- Social Functioning ScaleDokument7 SeitenSocial Functioning ScaleMihaela Cosmina NiculescuNoch keine Bewertungen
- Sheehan Anxiety ScaleDokument2 SeitenSheehan Anxiety ScaleSisy AnandaNoch keine Bewertungen
- 15 Mins RO-DBT Brief Intro Jan 2019Dokument13 Seiten15 Mins RO-DBT Brief Intro Jan 2019Momen ElghamrawyNoch keine Bewertungen
- Long-Term Consequences of Childhood Sexual Abuse by Gender of VictimDokument9 SeitenLong-Term Consequences of Childhood Sexual Abuse by Gender of VictimMalyasree BasuNoch keine Bewertungen
- Individual Values Assessment - An UpdateDokument3 SeitenIndividual Values Assessment - An Updatedarff45Noch keine Bewertungen
- DSM IV CodesDokument16 SeitenDSM IV CodesporzelNoch keine Bewertungen
- Reality TherapynicoleDokument30 SeitenReality Therapynicoleapi-267074391Noch keine Bewertungen
- Worksheets From The BFRB Recovery WorkbookDokument64 SeitenWorksheets From The BFRB Recovery WorkbookMarla DeiblerNoch keine Bewertungen
- Teenage AnxietyDokument34 SeitenTeenage Anxietyamit100% (1)
- QS: Social Exchange Theory: FoundersDokument2 SeitenQS: Social Exchange Theory: FounderssoulxpressNoch keine Bewertungen
- DSM-5 and Culture - The Need To Move Towards A Shared Model of Care Within A More Equal Patient-Physician PartnershipDokument3 SeitenDSM-5 and Culture - The Need To Move Towards A Shared Model of Care Within A More Equal Patient-Physician PartnershipPearl SkyNoch keine Bewertungen
- Assessment ToolsDokument74 SeitenAssessment ToolsSharvari ShahNoch keine Bewertungen
- Symptom Overreporting and Dissociative Experiences: A Qualitative ReviewDokument13 SeitenSymptom Overreporting and Dissociative Experiences: A Qualitative ReviewKamiNoch keine Bewertungen
- Executive Function Skills Questionnaire PDFDokument2 SeitenExecutive Function Skills Questionnaire PDFNikaelly LagesNoch keine Bewertungen
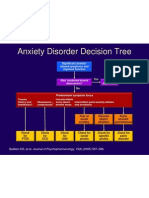
- Anxiety Disorder Decision TreeDokument1 SeiteAnxiety Disorder Decision Treecora4eva5699Noch keine Bewertungen
- Work Effectively in Trauma Informed CareDokument20 SeitenWork Effectively in Trauma Informed CareCharlie HaddadNoch keine Bewertungen
- T Alimentacion LibroDokument485 SeitenT Alimentacion LibrodeadelcarmenNoch keine Bewertungen
- 45 Psychological Testing SchwartzDokument25 Seiten45 Psychological Testing Schwartzumusulaimu mustafaNoch keine Bewertungen
- Teenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenVon EverandTeenage Health Concerns: How Parents Can Manage Eating Disorders In Teenage ChildrenNoch keine Bewertungen
- Behind the Therapy Door: Simple Strategies to Transform Your LifeVon EverandBehind the Therapy Door: Simple Strategies to Transform Your LifeNoch keine Bewertungen
- Personality and Arousal: A Psychophysiological Study of Psychiatric DisorderVon EverandPersonality and Arousal: A Psychophysiological Study of Psychiatric DisorderNoch keine Bewertungen
- BKTDokument36 SeitenBKTPriya PuriNoch keine Bewertungen
- Baumrind - S Parenting StylesDokument15 SeitenBaumrind - S Parenting StylesPriya Puri100% (1)
- Chapter 3 - Methodology: 3.1 RESEARCH DESIGN: A Before-After Experimental Design With Controls WasDokument17 SeitenChapter 3 - Methodology: 3.1 RESEARCH DESIGN: A Before-After Experimental Design With Controls WasPriya Puri100% (1)
- PsychoeducationDokument50 SeitenPsychoeducationPriya PuriNoch keine Bewertungen
- Adlerian TherapyDokument23 SeitenAdlerian TherapyPriya PuriNoch keine Bewertungen
- Guide For Carers - Supporting and Caring For A Person With Depression Anxiety and or A Related DisorderDokument44 SeitenGuide For Carers - Supporting and Caring For A Person With Depression Anxiety and or A Related DisorderPriya PuriNoch keine Bewertungen
- Community Mental Health Past, Present and Future in IndiaDokument5 SeitenCommunity Mental Health Past, Present and Future in IndiaPriya PuriNoch keine Bewertungen
- Plan of DissertationDokument27 SeitenPlan of DissertationPriya PuriNoch keine Bewertungen
- Social Phobia ManualDokument64 SeitenSocial Phobia Manualdroit33Noch keine Bewertungen
- Generalized Anxiety Disorder - Patient Treatment ManualDokument72 SeitenGeneralized Anxiety Disorder - Patient Treatment ManualPriya Puri100% (1)
- Journal Club: Institute of Psychiatry, KolkataDokument24 SeitenJournal Club: Institute of Psychiatry, KolkataPriya PuriNoch keine Bewertungen
- General Health QuestionnaireDokument3 SeitenGeneral Health QuestionnairePriya Puri60% (5)
- Parental Authority QuestionnaireDokument3 SeitenParental Authority QuestionnairePriya Puri100% (3)
- Beck Insight ScaleDokument11 SeitenBeck Insight ScalePriya PuriNoch keine Bewertungen
- Group Therapy Seminar 08-04-13Dokument64 SeitenGroup Therapy Seminar 08-04-13Priya Puri100% (1)
- Williams Emotional Stroop Test 1996Dokument22 SeitenWilliams Emotional Stroop Test 1996Priya PuriNoch keine Bewertungen
- Borderline Personality DisorderDokument44 SeitenBorderline Personality DisorderDean Amory100% (9)
- De Guzman Final ExamDokument6 SeitenDe Guzman Final ExamAlexa De GuzmanNoch keine Bewertungen
- Realism in R. K. Narayan's NovelsDokument27 SeitenRealism in R. K. Narayan's NovelsSharifMahmud75% (4)
- Docs of Catholic Church On Mission SummaryDokument11 SeitenDocs of Catholic Church On Mission SummaryVikash SharmaNoch keine Bewertungen
- Prophetic ProtocolDokument36 SeitenProphetic ProtocolNeil SoansNoch keine Bewertungen
- Nature of The ConstitutionDokument17 SeitenNature of The ConstitutionGrace MugorondiNoch keine Bewertungen
- Sample Tribute To ParentsDokument2 SeitenSample Tribute To ParentsYES O DavNorNoch keine Bewertungen
- SivamayamDokument2 SeitenSivamayamsmsekarNoch keine Bewertungen
- Flood Pre AdamicDokument31 SeitenFlood Pre AdamicEfraim MoraesNoch keine Bewertungen
- 182 - GE8076, GE6075 Professional Ethics in Engineering - Important QuestionsDokument16 Seiten182 - GE8076, GE6075 Professional Ethics in Engineering - Important QuestionsBhuvaneshNoch keine Bewertungen
- Nritya Ratna KoshaDokument9 SeitenNritya Ratna KoshaMedhaShahNoch keine Bewertungen
- Sophocles King OedipusDokument22 SeitenSophocles King OedipusRura more100% (1)
- Letter of Peter To PhilipDokument3 SeitenLetter of Peter To PhilipNightshade Wolfstone-FrancisNoch keine Bewertungen
- 2nd Tongues WorkshopDokument9 Seiten2nd Tongues WorkshopGary GumpalNoch keine Bewertungen
- 1st Quarter 2016 Lesson 4 Powerpoint With Tagalog NotesDokument25 Seiten1st Quarter 2016 Lesson 4 Powerpoint With Tagalog NotesRitchie FamarinNoch keine Bewertungen
- Church History Term PaperDokument8 SeitenChurch History Term Paperea7w32b0100% (1)
- Bible Quiz Questions-Acts 1Dokument2 SeitenBible Quiz Questions-Acts 1iamdeboz100% (2)
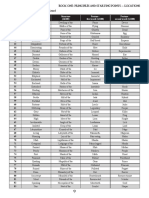
- ToAD Locations d100 Table 2Dokument1 SeiteToAD Locations d100 Table 2Walter Plum100% (1)
- Senarai Nama Buddy TerkiniDokument14 SeitenSenarai Nama Buddy TerkiniYap Yu SiangNoch keine Bewertungen
- Answer To RumiDokument6 SeitenAnswer To RumiE. Laurence BakeNoch keine Bewertungen
- Saudi Arabia Business Etiquette and Protocol GuideDokument0 SeitenSaudi Arabia Business Etiquette and Protocol GuideGlobal NegotiatorNoch keine Bewertungen
- RSCM Vol8issue1Dokument12 SeitenRSCM Vol8issue1api-245071749Noch keine Bewertungen
- ISB 542 Introduction To Fiqh Muamalat: The Concept of Property (Al-Maal) in IslamDokument22 SeitenISB 542 Introduction To Fiqh Muamalat: The Concept of Property (Al-Maal) in IslamsophiaNoch keine Bewertungen
- Biometrics and The Mark of The BeastDokument16 SeitenBiometrics and The Mark of The BeastTimothy100% (2)
- DVH Session 8Dokument22 SeitenDVH Session 8rajsab20061093100% (1)
- Khabs and KhuDokument20 SeitenKhabs and KhuSerraji MaxNoch keine Bewertungen
- Working Children's Movements in PeruDokument85 SeitenWorking Children's Movements in PeruPaul Cardan100% (1)
- Agehananda Bharati The Tantric Tradition PDFDokument347 SeitenAgehananda Bharati The Tantric Tradition PDFanatugario100% (1)
- Nil Santiáñez. Topographies of FascismDokument5 SeitenNil Santiáñez. Topographies of Fascismgbaeza9631Noch keine Bewertungen
- Paul's QualificationDokument10 SeitenPaul's QualificationKiran DNoch keine Bewertungen
- Repent To AllahDokument3 SeitenRepent To AllahIsnihaya Bint Mohammad RasumanNoch keine Bewertungen