Beruflich Dokumente
Kultur Dokumente
Muscular Dystrophy Types, Causes, Symptoms & Treatments
Hochgeladen von
vijay1234568883Originalbeschreibung:
Originaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Muscular Dystrophy Types, Causes, Symptoms & Treatments
Hochgeladen von
vijay1234568883Copyright:
Verfügbare Formate
MUSCULAR DYSTROPHY
INTRODUCTIO N
1|Page
MUSCULAR DYSTROPHY
INTRODUCTION
Muscular dystrophy (abbreviated MD) refers to a group of muscle diseases that weaken the muscles that move the human body. Muscular dystrophies are characterized by progressive skeletal muscle weakness, defects in muscle proteins, and the death of muscle cells and tissue. Nine diseases including Duchenne, Becker, limb girdle, congenital, facioscapulohumeral, myotonic, oculopharyngeal, distal, and Emery-Dreifuss are always classified as muscular dystrophy but there are more than 100 diseases in total with similarities to muscular dystrophy. Most types of MD are multi-system disorders with manifestations in body systems including the heart, gastrointestinal and nervous systems, endocrine glands, skin, eyes and other organs, namely the brain. The condition may also lead to mood swings and learning difficulties. In the 1860s, descriptions of boys who grew progressively weaker, lost the ability to walk, and died at an early age became more prominent in medical journals. In the following decade, French neurologist Guillaume Duchenne gave a comprehensive account of 13 boys with the most common and severe form of the disease (which now carries his name Duchenne muscular dystrophy). It soon became evident that the disease had more than one form, and that these diseases affected males of all ages. Muscular dystrophy (MD) is a genetic (inherited) condition that over time gradually causes the muscles to weaken. This leads to an increasing level of disability.
2|Page
MUSCULAR DYSTROPHY
There are several different types of MD, with different symptoms and patterns of progression. Not all types of MD cause severe disability, but there is currently no cure for the condition. MD is caused by mutations (cellular changes) in the genes that are responsible for the structure and functioning of a persons muscles. The mutations can occur spontaneously, but they are normally inherited from a persons parents. The mutations cause changes in the muscle fibres, which interferes with the muscles ability to function. Over time, this causes increasing disability. Muscular dystrophies are a group of inherited muscle disorders in which one or more genes needed for normal muscle function are defective, leading to muscle weakness (see Symptoms and Diagnosis of Musculoskeletal Disorders: Weakness) of varying severity. Other inherited muscle disorders include congenital myopathies, periodic paralysis, and glycogen storage diseases. Glycogen storage diseases are a group of rare inherited disorders in which muscles cannot metabolize sugars normally (see Hereditary Metabolic Disorders: Glycogen Storage Diseases), so they build up large stores of glycogen (a starch that is formed from sugars). Muscular dystrophy is the term used to describe a group of diseases of the muscles. With muscular dystrophy the muscles become weak and can waste away.There are over 20 different kinds of muscular dystrophies. The number of people affected by muscular dystrophy depends on the specific type. For example,approximately one child in 4,000 will have Spinal Muscular Atrophy.
3|Page
MUSCULAR DYSTROPHY
Approximately one in 3,000 will have Duchenne Muscular Dystrophy. The different types of muscular dystrophy have different causes. Some have genetic causes. A virus or illness causes some. Others have unknown causes.
To diagnose muscular dystrophy a doctor will take a detailed history, perform a thorough physical examination, and conduct specific tests. One of these tests is an electromyogram (EMG), which measuresthe electrical activity of the muscles.
If a diagnosis cannot be made based on these tests, a muscle biopsy is oftenThese tests usually give the diagnosis in about 80% of the patients. However, even with new tests approximately 15%-20% of patients will go undiagnosed.
Some of the health problems that people with muscle diseases can experience are problems with breathing and/or heart problems. Many patients can develop curvature of the spine (scoliosis) or muscle contractions leading to the need for surgery.
The treatment depends upon the specific cause of muscle weakness. However, physical therapy and occupational therapy are often used. In some cases a person with a muscle disease will get worse over time, and may have a shorter life expectancy than someone without the disease. However, some of the muscle diseases do not affect life expectancy at all.
4|Page
MUSCULAR DYSTROPHY
DEFINITION
5|Page
MUSCULAR DYSTROPHY
DEFINITION:One of a group of genetic diseases characterized by progressive weakness and degeneration of the skeletal or voluntary muscles which control movement. The muscles of the heart and some other involuntary muscles are also affected in some forms of muscular dystrophy, and a few forms involve other organs as well. Guillaume-Benjamin-Amand Duchenne, 1987 Inherited disease that causes progressive weakness in the skeletal (and occasionally heart) muscle. Muscle tissue degenerates and regenerates randomly and is replaced by scar tissue and fat. Britannica Concise Encyclopaedia, 1999 Muscular dystrophies (MD) are inherited disorders characterized by progressive weakness and degeneration of the skeletal or voluntary muscles which control movement, without a central or peripheral nerve abnormality. The muscles of the heart and other involuntary muscles are also affected in some forms of MD, and a few forms involve other organs as well. Neurological Disorder Journals, 2000
6|Page
MUSCULAR DYSTROPHY
REVIEW OF LITERATURE
ABSTRACT
7|Page
MUSCULAR DYSTROPHY
Lunt and Harper et al (1991) concluded that there is a dominantly inherited scapulohumeral or scapuloperoneal syndrome genetically distinct from FSHD that does not have facial weakness as a feature. Many cases (as much as 25%) may represent new, ex-novo mutations. Alan E H Emery et al 1954 stated that muscular dystrophies are a group of genetic diseases that severely affect children and adults. For sufferers and their family, the illness presents enormous physical and psychological challenges.
C. Jimenez-Mallebrera, S. C. Brown, C. A. Sewry and F. Muntoni et al December 2004 congenital muscular dystrophies are a clinically and genetically heterogeneous group of neuromuscular disorders. Each form has a characteristic phenotype, but there is overlap between some entities and their classification is based on a combination of clinical features and the primary or secondary protein defect.
Josef Finsterer et al 17 July 2006 becomes definite in all patients with MD, BMD, and MMP, but progresses markedly only in BMD patients within 10 years. MD, BMD, or MMP patients should be cardiologically investigated as soon as the neurological diagnosis is established and treated if CI becomes symptomatic, or in case of severe ECG or echocardiographic abnormalities.
8|Page
MUSCULAR DYSTROPHY
Stamulumab et al 2005/2006 trial was completed by Wyeth in Collegeville, PA. As of April 2007, the results of the study have not yet been made public, but it is one of the few known drugs in development for the treatment for muscular dystrophy. Myostatin is a protein that inhibits the growth of muscle tissue, MYO029 is a recombinant human antibody designed to bind and inhibit the activity of myostatin. Abu-Baker A, Rouleau GA et al 2003 made experiments and finally made a conculsion that Oculopharyngeal muscular dystrophy (OPMD) is an adult-onset disorder characterized by progressive eyelid drooping, swallowing difficulties and proximal limb weakness. OPMD is caused by a small expansion of a short polyalanine tract in the poly (A) binding protein nuclear 1 protein (PABPN1). QH Leyten et al 1996 Congenital muscular dystrophy (CMD) is a condition in which there are already at birth, marked hypotonia, generalized muscle weakness and frequently multiple contractures. CMD has recently been classified into four categories: CMD I, the classical or pure CMD without severe impairment of intellectual development; CMD II, the Fukuyama type CMD with muscle and structural brain abnormalities. B. G. M. van Engelen et al 16 December 1999 Central nervous system (CNS) characteristics were examined in seventeen patients with autosomal recessive classic or pure congenital muscular dystrophy (CMD). In three patients, neuroradiological examination (CT/MRI) indicated hypodense white matter areas. Two out of these three patients had epilepsy (seizures and epileptic discharges on their EEG)
9|Page
MUSCULAR DYSTROPHY
F. J. M. Gabrels et al 19 March 1999 conducted an experiment on congenital muscular dystrophy (CMD) in a 13-year-old girl with early manifestation of muscle weakness and hypotonia, severe contractures, bulbar syndrome, progressive external ophtalmoplegia, and white matter changes on magnetic resonance imaging (MRI) of the brain, but no mental defect. Serum creatine kinase (CK) level was normal. Jennifer E. Morgan et al 26 August 2002 observed that Steroids represent the only pharmacological palliative treatment for Duchenne muscular dystrophy. However, they do have side effects and despite a large number of published studies showing their efficacy, they are still not universally used. This is largely due to the lack of functional outcome and quality of life measures in most of the published studies and suggests that further trials might be required to answer some of the still unclear aspects of their role. Sara T Winokur et al 19 November 2002 reported that the myoblasts suggests that aberrant gene expression occurs early in facioscapulohumeral muscular dystrophy muscle development. In order to test this hypothesis, global gene expression profiling and in vitro characterization of facioscapulohumeral muscular dystrophy and control myoblasts were carried out. Silvre M. van der Maarel et al 30 May 2006 Clinical trials based on suppression of inflammatory reactions or increasing muscle mass by drugs or training have been disappointing. A recent, probably the first evidence-based pilot trial to revert epigenetic changes did also not provide grounds for a larger clinical study. Clearly, better disease models need to be developed to identify and test novel intervention strategies to eventually improve the quality of life for patients with FSHD.
10 | P a g e
MUSCULAR DYSTROPHY
Rabi Tawil et al 3 October 2008 reveals that Autosomal dominant facioscapulohumeral muscular dystrophy (FSHD) is mainly characterized by progressive wasting and weakness of the facial, shoulder, and upper-arm muscles. FSHD is caused by contraction of the macrosatellite repeat D4Z4 on chromosome 4q35. The D4Z4 repeat is very polymorphic in length, and D4Z4 rearrangements occur almost exclusively via intrachromosomal gene conversions. H. Lidov et al manufestated a prototypical form is Duchenne muscular dystrophy, an X-linked disorder, but there are nearly 20 rarer similar disorders called limbgirdle dystrophies or congenital muscular dystrophies. Duchenne dystrophy is caused by loss of dystrophin, a 427 kDa cytoskeletal actin-binding protein. A cluster of proteins that form an integral membrane complex (dystroglycans, sarcoglycans) links dystrophin to the extracellular matrix. Kate Bushby et al 27 September 2006 stated that The limb-girdle muscular dystrophies are a group of disorders where our understanding of their underlying molecular basis has made huge strides over the past years, revealing great heterogeneity at the clinical and molecular level.
11 | P a g e
MUSCULAR DYSTROPHY
TYPES
Types
12 | P a g e
MUSCULAR DYSTROPHY
1. 2. 3. 4. 5. 6. 7. 8. 9. 10.
Duchenne muscular dystrophy Becker's muscular dystrophy Congenital muscular dystrophy Distal muscular dystrophy Emery-Dreifuss muscular dystrophy Facioscapulohumeral muscular dystrophy Limb-girdle muscular dystrophy Myotonic muscular dystrophy Oculopharyngeal muscular dystrophy Spinal muscular atrophy
Duchenne muscular dystrophy (DMD)
13 | P a g e
MUSCULAR DYSTROPHY
Duchenne muscular dystrophy (DMD) is a severe recessive X-linked form of muscular dystrophy characterized by rapid progression of muscle degeneration, eventually leading to loss of ambulation and death. This affliction affects one in 3500 males, making it the most prevalent of muscular dystrophies. In general, only males are afflicted, though females can be carriers. Females may be afflicted if the father is afflicted and the mother is also a carrier/ affected. The disorder is caused by a mutation in the gene DMD, located in humans on the X chromosome (Xp21). The DMD gene codes for the protein dystrophin, an important structural component within muscle tissue. Dystrophin provides structural stability to the dystroglycan complex (DGC), located on the cell membrane. Symptoms usually appear in male children before age 5 and may be visible in early infancy. Progressive proximal muscle weakness of the legs and pelvis associated with a loss of muscle mass is observed first. Eventually this weakness spreads to the arms, neck, and other areas. Early signs may include pseudohypertrophy (enlargement of calf and deltoid muscles), low endurance, and difficulties in standing unaided or inability to ascend staircases. As the condition progresses, muscle tissue experiences wasting and is eventually replaced by fat and fibrotic tissue (fibrosis). By age 10, braces may be required to aid in walking but most patients are wheelchair dependent by age 12. Later symptoms may include abnormal bone development that lead to skeletal deformities, including curvature of the spine. Due to progressive deterioration of muscle, loss of movement occurs eventually leading to paralysis. Intellectual impairment may or may not be present but if present, does not progressively worsen as the child ages.
Becker's muscular dystrophy
14 | P a g e
MUSCULAR DYSTROPHY
A form of muscular dystrophy that is quite similar to Duchenne muscular dystrophy, except that patients with Becker do produce some of the key protein, dystrophin, whereas those with Duchenne do not. Progression of the disease in Becker type is slower than in Duchenne, and symptoms may appear as late as the mid-twenties. Becker muscular dystrophy (also known as Benign pseudohypertrophic muscular dystrophy) is an X-linked recessive inherited disorder characterized by slowly progressive muscle weakness of the legs and pelvis. It is a type of dystrophinopathy, which includes a spectrum of muscle diseases in which there is insufficient dystrophin produced in the muscle cells, resulting in instability in the structure of muscle cell membrane. This is caused by mutations in the dystrophin gene, which encodes the protein dystrophin. Becker muscular dystrophy is related to Duchenne muscular dystrophy in that both result from a mutation in the dystrophin gene, but in Duchenne muscular dystrophy no functional dystrophin is produced making DMD much more severe than BMD. Both Duchenne and Becker muscular dystrophy have traditionally been called "Xlinked" recessive diseases, but in view of modern molecular biology and identification of the dystrophin gene, it might be more appropriate to say they are X-chromosome recessive diseases.
15 | P a g e
MUSCULAR DYSTROPHY
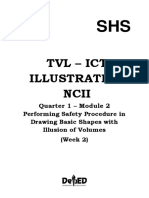
Figure No-1.1 shows the involvement of body parts for Duchenne and Beckers type.
Congenital muscular dystrophy
16 | P a g e
MUSCULAR DYSTROPHY
Congenital muscular dystrophy (CMD) is the term used to describe muscular dystrophy that is present at birth. CMD describes a number of autosomal recessive diseases of muscle weakness and possible joint deformities, present at birth and slowly progressing. Life expectancies for affected individuals vary, although some forms of CMD do not affect life span at all. All such known dystrophies are genetically recessive and result from mutations in a variety of different genes, including those encoding the laminin-2 chain, fukutin-related protein, LARGE and fukutin, amongst others. Currently there is no cure. Physical and occupational therapy, surgery, wheelchairs and other assistive technology may be helpful. Congenital myopathies (including X-linked myotubular myopathy and nemaline myopathy) typically have normal or near-normal serum CK concentration and evidence of developmental rather than dystrophic muscle abnormalities on muscle biopsy. Congenital muscular dystrophy type 1C (MDC1C). MDC1C is a severe form of CMD with partial merosin deficiency and a partial deficiency of alpha dystroglycan. This form of CMD has been mapped to chromosome 19q13.3 with homozygous mutations identified in the FKRP gene. Mutations in this 12-kb gene, which is composed of three non-coding exons and one large coding exon, is also the cause of LGMD2I (see Limb-Girdle Muscular Dystrophy Overview), which, despite a variable phenotype, is milder in presentation than MDC1C. While one common mutation has been identified in FKRP, this mutation has only been observed in persons with LGMD2I and has not been seen in MDC1C. Brown et al (2004) correlated both the mutation type and expression of alpha
17 | P a g e
MUSCULAR DYSTROPHY
dystroglycan with the disease phenotype. Specifically, persons with MDC1C consistently show a severe deficiency of alpha dystroglycan and are either compound heterozygotes for one missense mutation and one nonsense mutation or have two missense mutations. Conversely, individuals with LGMD2I have the common mutation (C826A) and either a missense or nonsense mutation, and only mild to moderately decreased alpha dystroglycan. Individuals with mild LFMD2I are homozygous for the common mutation and show only a mild deficiency of alpha dystroglycan.
Distal muscular dystrophy
One of two genetic muscle diseases characterized by wasting of the muscles most distant from the midline, such as those of the hands and feet. Both types of distal
18 | P a g e
MUSCULAR DYSTROPHY
MD are inherited in an autosomal dominant manner and may affect males and females. The first type of distal MD starts in infancy, does not progress after adolescence, and is not debilitating. The second type of distal MD starts after age 40, affects the muscles of the hands and feet and then the muscles closer to the trunk but does not shorten the life span.
Emery-Dreifuss muscular dystrophy
Abbreviated EDMD. A form of muscular dystrophy that begins in childhood or adolescence as a slowly progressive disorder of the upper arms or upper legs characterized by weakness and atrophy of muscles without involvement of the nervous system. Contractures of the limbs, especially the elbows, are common complications, as are serious heart problems. EDMD is caused by mutation in the gene encoding emerin in chromosome band Xq28. Although only males have the muscle problems associated with EDMD, females may have the heart problems. Accordingly, female relatives of males with this disorder should have regular heart check-ups. There are two other known types of EDMD. Both are caused by mutation in the lamin A gene (LMNA). One displays similar features to EDMD and is inherited in an autosomal dominant manner; it is classified as EDMD type 2. The other type appears to lack cardiac problems and is inherited in an autosomal recessive manner; it is EDMD type 3. Mutations in the EMD and LMNA genes cause Emery-Dreifuss muscular dystrophy. The EMD and LMNA genes provide instructions for making proteins
19 | P a g e
MUSCULAR DYSTROPHY
that are components of the nuclear envelope, which surrounds the nucleus in cells. The nuclear envelope regulates the movement of molecules into and out of the nucleus, and researchers believe it may play a role in regulating the activity of certain genes.
Most cases of Emery-Dreifuss muscular dystrophy are caused by mutations in the EMD gene. This gene provides instructions for making a protein called emerin, which appears to be essential for the normal function of skeletal and cardiac muscle. Most EMD mutations prevent the production of any functional emerin. It remains unclear how a lack of this protein results in the signs and symptoms of Emery-Dreifuss muscular dystrophy.
Less commonly, Emery-Dreifuss muscular dystrophy results from mutations in the LMNA gene. This gene provides instructions for making two very similar proteins, lamin A and lamin C. Most of the LMNA mutations that cause this condition result in the production of an altered version of these proteins.
20 | P a g e
MUSCULAR DYSTROPHY
Figure No-1.2 shows the involvement of body parts for Emery-Dreifuss muscular dystrophy.
21 | P a g e
MUSCULAR DYSTROPHY
Facioscapulohumeral muscular dystrophy
A form of muscular dystrophy that begins before age 20 with slowly progressive weakness of the muscles of the face, shoulders, and feet. The severity of the disease is variable. Although most people with facioscapulohumeral muscular dystrophy (FSHD) retain the ability to walk, about 20% of affected individuals require a wheelchair. Life expectancy is not shortened. The diagnosis of FSHD can be confirmed by a DNA test disclosing the deletion of copies of a repeat motif called D4Z4 on chromosome 4. FSHD is inherited in an autosomal dominant manner. Offspring of an affected individual have a 50% chance of inheriting the mutant at 4. About 10-30% of cases are due to a new mutation. Prenatal testing is available.
More than 95% of cases of FSHD are associated with the deletion of integral copies of a tandemly repeated 3.2kb unit (D4Z4 repeat) at the subtelomeric region 4q35 of the Human genome of which a normal chromosome will include between 11-150 repetitions of D4Z4.
There are both heterochromatin and euchromatin structures within D4Z4 and one putative gene called DUX4. Inheritance is autosomal dominant, though up to one-third of the cases appear to be the result of de novo (new) mutations. The heterochromatin is specifically lost in the deletions of FSHD while the euchromatin structures remain.
If the entire region is removed, there are birth defects, but no specific defects on skeletal muscle.
Individuals appear to require the existence of 11 or fewer repeat units to be at risk for FSHD. Though the nature of the DNA mutation is known, it has
22 | P a g e
MUSCULAR DYSTROPHY
not been possible to identify a gene or mechanism that causes FSHD and a novel position effect has been postulated to explain the disease phenotype. In addition, a few cases of FSHD are the result of rearrangements between subtelomeric chromosome 4q and a subtelomeric region of 10q. This location contains a tandem repeat structure highly homologous to 4q35.
Disease occurs when the translocation results in a critical loss of tandem repeats to the 4q site.
23 | P a g e
MUSCULAR DYSTROPHY
Figure no-1.3 shows the involvement of body parts for Facioscapulohumeral muscular dystrophy.
24 | P a g e
MUSCULAR DYSTROPHY
Limb-girdle muscular dystrophy
Limb-girdle muscular dystrophy or Erb's muscular dystrophy is an autosomal class of muscular dystrophy that is similar but distinct from Duchenne muscular dystrophy and Becker's muscular dystrophy. Limbgirdle muscular dystrophy encompasses a large number of rare disorders.
The term "limb-girdle" is used to describe these disorders because the muscles most severely affected are generally those of the hips and shoulders -- the limb girdle muscles.
Common symptoms of limb-girdle muscular dystrophy are muscle weakness, myoglobinuria, pain, myotonia, cardiomyopathy, elevated serum CK, and rippling muscles.
The muscle weakness is generally symmetric, proximal, and slowly progressive.
In most cases, pain is not present with LGMD, and mental function is not affected. LGMD can begin in childhood, adolescence, young adulthood or even later. The age of onset is usually between 10 and 30. Both genders are affected equally. When limb-girdle muscular dystrophy begins in childhood the progression appears to be faster and the disease more disabling. When the disorder begins in adolescence or adulthood the disease is generally not as severe and progresses more slowly. There is no sensory neuropathy or autonomic or visceral disfunction at presentation.the specific dermatomes affected can be demonstrated clinically,and although lower limb deep tendon reflexes and plantar reflex are lost, abdominal reflexes are preserved
25 | P a g e
MUSCULAR DYSTROPHY
One of a group of diseases that may begin in childhood or later with slowly progressive weakness and wasting of the muscles restricted to the limb musculature, especially to the hips and shoulders. Muscle biopsies of the limb-girdle muscular dystrophies typically show degeneration and regeneration of muscle (dystrophic biopsy). There is usually an elevated CPK (creatine phosphokinase) in the blood. Most patients show relative sparing of the heart and bulbar muscles. The limb-girdle muscular dystrophies are caused a number of genetic defects and can affect both males and females. Inheritance is usually autosomal recessive or, more rarely, autosomal dominant.
Figure no-1.3 shows the involvement of body parts for Limb-girdle muscular dystrophy
26 | P a g e
MUSCULAR DYSTROPHY
Myotonic muscular dystrophy An inherited disease in which the muscles contract but have decreasing power to relax -- this phenomenon is termed myotonia (irritability and prolonged contraction of muscles). The disease also leads to a mask-like expressionless face, premature balding, cataracts, and heart arrhythmias (abnormalities in heart rhythm). The onset of such problems is usually in young adulthood. However, onset can be at any age and the disease is extremely variable in the degree of severity. Myotonic dystrophy is due to a trinucleotide repeat (a "stuttering" sequence of three bases) in the DNA. The myotonic dystrophy gene (called DM1), found on chromosome 19q13.3, codes for a protein kinase (an enzyme) that is found in skeletal muscle. An unusual feature is that the signs and symptoms of the disease usually become more severe with each successive generation. This is because mistakes in the faithful copying of the gene from one generation to the next result in the amplification of a genomic "AGC/CTG triplet repeat." Unaffected individuals have between 5 and 27 copies of AGC/CTG, myotonic dystrophy patients who are minimally affected have at least 50 repeats, while more severely affected patients have an expansion of up to several kilobase pairs.
27 | P a g e
MUSCULAR DYSTROPHY
Oculopharyngeal muscular dystrophy
A form of muscular dystrophy that begins in the muscles of the eyes and throat. It usually appears between the ages of 40 and 60, and progresses slowly. Oculopharyngeal muscular dystrophy is inherited in an autosomal dominant manner and affects both males and females. It may be more than one disease. One type is caused by mutation in the PABP2 gene on chromosome 14 encodes poly(A)-binding protein-2.
Figure no-1.4 shows the involvement of body parts for Oculopharyngeal muscular dystrophy
28 | P a g e
MUSCULAR DYSTROPHY
Spinal muscular atrophy
Spinal Muscular Atrophy (SMA) is a neuromuscular disease characterized by degeneration of motor neurons, resulting in progressive muscular atrophy (wasting away) and weakness. The clinical spectrum of SMA ranges from early infant death to normal adult life with only mild weakness. These patients often require comprehensive medical care involving multiple disciplines, including pediatric pulmonology, pediatric neurology, pediatric orthopedic surgery, Lower Extremity & Spinal Orthosis, pediatric critical care, and physical medicine and rehabilitation; and physical therapy, occupational therapy, respiratory therapy, and clinical nutrition. Genetic counseling is also helpful for the parents and family members. Sensation and the ability to feel are not affected. Intellectual activity is normal and it is often observed that patients with SMA are unusually bright and sociable. In all of its forms, the primary feature of SMA is muscle weakness, accompanied by atrophy of muscle. This is the result of denervation, or loss of the signal to contract, that is transmitted from the spinal cord. This is normally transmitted from motor neurons in the spinal cord to muscle via the motor neuron's axon, but either the motor neuron with its axon, or the axon itself, is lost in all forms of SMA. The features of SMA are strongly related to its severity and age of onset. SMA caused by mutation of the SMN gene has a wide range, from infancy to adult, fatal to trivial, with different affected individuals manifesting every shade of impairment between these two extremes. Many of the symptoms of SMA relate to secondary complications of muscle weakness, and as such can be at least partially remediated by prospective therapy.
29 | P a g e
MUSCULAR DYSTROPHY
Infantile SMA is the most severe form. Some of the symptoms include:
Muscle weakness Poor muscle tone Weak cough Limpness or a tendency to flop Difficulty sucking or swallowing Accumulation of secretions in the lungs or throat Bell-shaped torso, caused by breathing using muscles around the tummy area Clenched fists with sweaty hands Flickering/vibrating of the tongue Head often tilted to one side, even when lying down Legs that tend to be weaker than the arms Legs lying in the "frogs leg" position Hypotonia, areflexia, and multiple congenital contractures (arthrogryposis) associated with loss of anterior horn cells Feeding difficulties Increased susceptibility to respiratory tract infections Bowel/bladder weakness Lower-than-normal weight Developmental milestones, such as lifting the head or sitting up, can't be reached
30 | P a g e
MUSCULAR DYSTROPHY
AETIOLOGY
31 | P a g e
MUSCULAR DYSTROPHY
AETIOLOGY
All muscular dystrophies are inherited (genetic) conditions (even though some forms may form from an ex-novo mutation). Different muscular dystrophies follow various inheritance patterns:
Duchenne muscular dystrophy (DMD)
It is inherited in an X-linked recessive pattern, meaning that the mutated gene that causes the disorder is located on the X chromosome (one of the two sex chromosomes, the other being Y) and is thus considered sex-linked. In males (who have only one X chromosome) one altered copy of the gene in each cell is sufficient to cause the condition. In females (who have two X chromosomes) a mutation must generally be present in both copies of the gene to cause the disorder (relatively rare exceptions, manifesting carriers, do occur due to dosage compensation/X-inactivation). Males are therefore affected by X-linked recessive disorders much more often than females. A characteristic of X-linked inheritance is that fathers cannot pass Xlinked traits to their sons. In about two thirds of DMD cases, an affected male inherits the mutation from a mother who carries one altered copy of the DMD gene. The other one third of cases probably result from new mutations in the gene. Females who carry one copy of a DMD mutation may have some signs and symptoms related to the condition (such as muscle weakness and cramping), but these are typically milder than the signs and symptoms seen in affected males.
32 | P a g e
MUSCULAR DYSTROPHY
Duchenne muscular dystrophy and Becker's muscular dystrophy are caused by mutations of the gene for the dystrophin protein and lead to an overabundance of the enzyme creatine kinase.
Myotonic Muscular Dystrophy
Autosomal dominant pattern of inheritance. Myotonic dystrophy results from the expansion of a short repeat in the DNA sequence (CTG in one gene or CCTG in another gene). In other words, the the gene defect is an abnormally long repetition of a three- or four-letter "word" in the genetic code. While the exact mechanism of action is not known, this molecular change may interfere with the production of important muscle proteins
Limb-Girdle Muscular Dystrophy
Many forms of LGMD have been identified, showing different patterns of inheritance (autosomal recessive vs. autosomal dominant). In an autosomal recessive pattern of inheritance, an individual receives two copies of the defective gene, one from each parent. The recessive LGMDs are more frequent than the dominant forms. The dominant LGMDs usually show adult onset. Some of the recessive forms have been associated with defects in proteins that make up the dystrophin-glycoprotein complex. The term "limb-girdle" is used to describe these disorders because the muscles most severely affected are generally those of the hips and shoulders -- the limb girdle muscles.
33 | P a g e
MUSCULAR DYSTROPHY
The muscle weakness is generally symmetric, proximal, and slowly progressive. In most cases, pain is not present with LGMD, and mental function is not affected. LGMD can begin in childhood, adolescence, young adulthood or even later. The age of onset is usually between 10 and 30. Both genders are affected equally. When limb-girdle muscular dystrophy begins in childhood the progression appears to be faster and the disease more disabling. When the disorder begins in adolescence or adulthood the disease is generally not as severe and progresses more slowly.
There is no sensory neuropathy or autonomic or visceral disfunction at presentation.the specific dermatomes affected can be demonstrated clinically,and although lower limb deep tendon reflexes and plantar reflex are lost, abdominal reflexes are preserved
Congenital Muscular Dystrophy
Autosomal recessive or autosomal dominant; these diseases are sometimes inherited through both parents and sometimes inherited from one parent. They can also occur spontaneously because of a newly developed genetic mutation
Congenital muscular dystrophy (CMD) is the term used to describe muscular dystrophy that is present at birth. CMD describes a number of autosomal recessive diseases of muscle weakness and possible joint deformities, present at birth and slowly progressing. Life expectancies for affected individuals vary, although some forms of CMD do not affect life span at all.
34 | P a g e
MUSCULAR DYSTROPHY
All such known dystrophies are genetically recessive and result from mutations in a variety of different genes, including those encoding the laminin-2 chain, fukutin-related protein, LARGE and fukutin, amongst others. Currently there is no cure. Physical and occupational therapy, surgery, wheelchairs and other assistive technology may be helpful.
Distal Muscular Dystrophy
May be autosomal dominant, (a faulty gene is inherited from one parent); or autosomal recessive (when a faulty gene is inherited from both parents).
Distal muscular dystrophy (or distal myopathy) is a group of disorders characterized by onset in the hands or feet. Many types involve dysferlin, but it has been suggested that not all cases do
Facioscapulohumeral Muscular Dystrophy
More than 95% of cases of FSHD are associated with the deletion of integral copies of a tandemly repeated 3.2kb unit (D4Z4 repeat) at the subtelomeric region 4q35 of the Human genome of which a normal chromosome will include between 11-150 repetitions of D4Z4. There are both heterochromatin and euchromatin structures within D4Z4 and one putative gene called DUX4. Inheritance is autosomal dominant, though up to one-third of the cases appear to be the result of de novo (new) mutations. The heterochromatin is specifically lost in the deletions of FSHD while the euchromatin structures remain. If the entire region is removed, there are birth defects, but no specific defects on skeletal muscle. Individuals appear to require the existence of 11 or
35 | P a g e
MUSCULAR DYSTROPHY
fewer repeat units to be at risk for FSHD. Though the nature of the DNA mutation is known, it has not been possible to identify a gene or mechanism that causes FSHD and a novel position effect has been postulated to explain the disease phenotype. Emery-Dreifuss Muscular Dystrophy Can be X-linked recessive, primarily affecting males, who inherit the disease through their mothers. Another type is autosomal dominant, meaning it can be inherited through either parent; an autosomal recessive type occurs when a faulty gene is inherited from both parents. Among the earliest features of this disorder are joint deformities called contractures, which restrict the movement of certain joints. Contractures become noticeable in early childhood to teenage years and most often involve the elbows, ankles, and neck. Most affected individuals also experience slowly progressive muscle weakness and wasting, beginning in muscles of the upper arms and lower legs and progressing to muscles in the shoulders and hips. A power chair or scooter or wheelchair may be needed by adulthood. Almost all people with Emery-Dreifuss muscular dystrophy have heart problems by adulthood. In many cases, these heart problems stem from abnormalities of the electrical signals that control the heartbeat (cardiac conduction defects) and abnormal heart rhythms (arrhythmias). If untreated, these abnormalities can lead to an unusually slow heartbeat (bradycardia), fainting (syncope), and an increased risk of stroke and sudden death. Oculopharyngeal Muscular Dystrophy
36 | P a g e
MUSCULAR DYSTROPHY
May be autosomal dominant, meaning OPMD is inherited from one parent; or autosomal recessive, occurring when a faulty gene is inherited from each parent.
Abnormal vacuoles within muscle fibres. A distinction between OPD and myasthenia gravis or mitochondrial myopathy must be made. The absence of family history and the fluctuation of symptoms in myasthenia gravis usually distinguish the two conditions
37 | P a g e
MUSCULAR DYSTROPHY
PATHOPHYSIOLOGY
Duchenne muscular dystrophy and Becker muscular dystrophy:Devastating inherited neuromuscular disorder that affects one in 3300 live male births. Although the responsible gene and its product, dystrophin, have been characterized for more than 15 years, and a mouse model (mdx) has been developed, comprehensive understanding of the mechanism leading from the
38 | P a g e
MUSCULAR DYSTROPHY
absence of dystrophin to the muscular degeneration is still debated. First, dystrophin is considered a key structural element in the muscle fiber, and the primary function of the dystrophin-associated protein complex is to stabilize plasma membrane, although a role of signaling is still possible. Mechanically induced damage through eccentric contractions puts a high stress on fragile membranes and provokes micro-lesions that could eventually lead to loss of calcium homeostasis, and cell death. Altered regeneration, inflammation, impaired vascular adaptation, and fibrosis are probably downstream events that take part in the muscular dystrophy and that probably vary a lot along species (i.e., mdx mice), probands within families, stressing the importance of epigenic factors.
Because no etiologic therapy is available for Duchenne muscular dystrophy, a better understanding of the primary and downstream mechanisms could prove useful for producing new adjuvant treatments. All pathophysiologic mechanisms are reviewed together with perspectives on management.
Facioscapulohumeral muscular dystrophy
The exact pathophysiology of FSHD remains unknown as of March 2007. Muscle histologic changes are nonspecific for the muscle wasting. There is evidence of early inflammatory changes in the muscle, but reported responses to high dose open labeled corticosteroid treatment have been negative. Animal studies of anabolic effects of beta adrenergic agonists on models of muscle wasting led to an
39 | P a g e
MUSCULAR DYSTROPHY
open trial of albuterol (a beta adrenergic agonist) in which limited preliminary results support an improvement of muscle mass and strength in FSHD. Preliminary studies of muscle cultures suggest an increased sensitivity to oxidative stress, but require further exploration.
Myotonic dystrophy
Myotonic dystrophy (DM) is a clinically and genetically heterogeneous disorder. There are two major forms: DM1, for a century known as Steinert's disease DM2, recognized in 1994 as a milder version of DM1. These autosomal dominant conditions are among the most common forms of adultonset muscular dystrophy. However, DM is more than simply a muscular dystrophy per se, since affected individuals may show cataracts, cardiac conduction abnormalities, infertility, and insulin resistance. Furthermore, there is a severe congenital form of DM1 with marked developmental disability.
Limb-girdle muscular dystrophy
It is typically an inherited disorder, though it may be inherited as a dominant, recessive, or X-linked genetic defect. The result of the defect is that the muscles cannot properly form the proteins needed for normal muscle function. Several different proteins can be affected, and the specific protein that is absent or defective identifies the specific type of muscular dystrophy.
40 | P a g e
MUSCULAR DYSTROPHY
Emery-Dreifuss muscular dystrophy
Mutations in the EMD and LMNA genes cause Emery-Dreifuss muscular dystrophy. The EMD and LMNA genes provide instructions for making proteins that are components of the nuclear envelope, which surrounds the nucleus in cells. The nuclear envelope regulates the movement of molecules into and out of the nucleus, and researchers believe it may play a role in regulating the activity of certain genes. Most cases of Emery-Dreifuss muscular dystrophy are caused by mutations in the EMD gene. This gene provides instructions for making a protein called emerin, which appears to be essential for the normal function of skeletal and cardiac muscle. Most EMD mutations prevent the production of any functional emerin. It remains unclear how a lack of this protein results in the signs and symptoms of Emery-Dreifuss muscular dystrophy. Less commonly, Emery-Dreifuss muscular dystrophy results from mutations in the LMNA gene. This gene provides instructions for making two very similar proteins, lamin A and lamin C. Most of the LMNA mutations that cause this condition result in the production of an altered version of these proteins.
SIGNS
41 | P a g e
MUSCULAR DYSTROPHY
AND SYMPTOMS
42 | P a g e
MUSCULAR DYSTROPHY
Signs and symptoms Main symptoms include:
Progressive muscular wasting Poor balance Frequent falls Walking difficulty Waddling gait Calf deformation Limited range of movement Respiratory difficulty Drooping eyelids Gonadal Loss of bladder control Scoliosis (curvature of the spine and the back) Inability to walk
Few or none of these symptoms may be present before diagnosis. Some types of muscular dystrophy can affect the heart, causing cardiomyopathy or arrhythmias
NOTE: There are different types of muscular dystrophy, each affecting different sets of muscles and resulting in different degrees of muscle weakness.
Type of Muscular Dystrophy
Description
Symptoms
43 | P a g e
MUSCULAR DYSTROPHY Duchenne muscular dystrophy most common and the most severe 1 out of every 3,500 boys (Girls can carry the gene that causes the disease, but they usually have no symptoms) begins to appear around age 5, as the pelvic muscles begin to weaken muscles weaken in the shoulders, back, arms, and legs eventually, the respiratory muscles are affected, and a ventilator is required to assist breathing kids: a life span of about 20 years, about one-third of them experience learning disabilities and a small Becker muscular dystrophy less common and progresses more slowly affects approximately 1 in 30,000 boys caused by insufficient production Myotonic dystrophy of dystrophin also known as Steinert's disease most common adult form of MD, although half of all cases are diagnosed in people under 20 years old caused by a portion of a particular gene that is larger than it Limb-girdle muscular dystrophy should be affects boys and girls equally usually begins when kids are between 8 and 15 years old progresses slowly, affecting the pelvic, shoulder, and back muscles severity of muscle weakness varies some kids have only mild weakness can appear at any time during a child's life muscle weakness, myotonia (in which the muscles have trouble relaxing once they contract), and muscle wasting, where the muscles shrink over time kids: can also experience cataracts and heart problems number having mental retardation begins during the teen years muscle weakness first begins in the pelvic muscles, then moves into the shoulders and back children: normal life span and can lead long, active lives without the use of a wheelchair
44 | P a g e
MUSCULAR DYSTROPHY while others develop severe disabilities and as adults need to use a Facioscapulohumeral muscular dystrophy can affect both boys and girls wheelchair first appears during the teen years tends to progress slowly muscle weakness first develops in the face, making it difficult for a child to close the eyes, whistle, or puff out the cheeks the shoulder and back muscles gradually become weak, and kids have difficulty lifting objects or raising their hands overhead over time, the legs and pelvic muscles also may lose strength
45 | P a g e
MUSCULAR DYSTROPHY
Figure no-1.6 shows the clinical features of the muscular dystrophy patient
First Symptoms
Many kids with muscular dystrophy follow a normal pattern of development
46 | P a g e
MUSCULAR DYSTROPHY
during their first few years of life. But in time common symptoms begin to appear. A child who has MD may start to stumble, waddle, have difficulty going up stairs, and toe walk (walk on the toes without the heels hitting the floor). A child may start to struggle to get up from a sitting position or have a hard time pushing things, like a wagon or a tricycle.
Kids with MD often develop enlarged calf muscles (called calf pseudo hypertrophy) as muscle tissue is destroyed and replaced by fat.
Gowers' sign is a medical sign that indicates weakness of the proximal muscles, namely those of the lower limb. The sign describes a patient that has to use his or her hands and arms to "walk" up his or her own body from a squatting position due to lack of hip and thigh muscle strength.
47 | P a g e
MUSCULAR DYSTROPHY
Figure no-1.6 shows the Gowers' sign
48 | P a g e
MUSCULAR DYSTROPHY
INVESTIGATIONS
INVESTIGATIONS DNA test The muscle-specific isoform of the dystrophin gene is composed of 79 exons, and DNA testing and analysis can usually identify the specific type of
49 | P a g e
MUSCULAR DYSTROPHY
mutation of the exon or exons that are affected. DNA testing confirms the diagnosis in most cases. Muscle biopsy If DNA testing fails to find the mutation, a muscle biopsy test may be performed. A small sample of muscle tissue is extracted (usually with a scalpel instead of a needle) and a dye is applied that reveals the presence of dystrophin. Complete absence of the protein indicates the condition. Over the past several years DNA tests have been developed that detect more of the many mutations that cause the condition, and muscle biopsy is not required as often to confirm the presence of Duchenne's. Serum creatine phosphokinase measurements: Serum creatine phosphokinase levels are more than 10 times in the elevated muscular dystrophy patients. Prenatal tests If one or both parents are 'carriers' of a particular condition, there is a risk that their unborn child will be affected by that condition. 'Prenatal tests' are carried out during pregnancy, to try to find out if the fetus (unborn child) is affected. The tests are only available for some neuromuscular disorders. Different types of prenatal tests can be carried out after about 11 weeks of pregnancy. Chorion villus sampling (CVS) can be done at 1114 weeks, and amniocentesis after 15 weeks, while fetal blood sampling can be done at about 18 weeks. Women and/or couples need to consider carefully which test to have and to discuss this with their genetic counselor. Earlier testing would allow early termination, but it carries a slightly higher risk of miscarriage than later testing (about 2%, as opposed to 0.5%).
50 | P a g e
MUSCULAR DYSTROPHY
51 | P a g e
MUSCULAR DYSTROPHY
MEDICAL MANAGEMENT
52 | P a g e
MUSCULAR DYSTROPHY
MEDICAL MANAGEMENT
There is no known cure for muscular dystrophy. Inactivity (such as bed rest and even sitting for long periods) can worsen the disease. Physical therapy, occupational therapy, orthotic intervention, speech therapy and orthopedic instruments (e.g., wheelchairs, standing frames) may be helpful. There is no specific treatment for any of the forms of muscular dystrophy. Physical therapy to prevent contractures and maintain muscle tone, orthoses (orthopedic appliances used for support) and corrective orthopedic surgery may be needed to improve the quality of life in some cases. The cardiac problems that occur with Emery-Dreifuss muscular dystrophy and myotonic muscular dystrophy may require a pacemaker. The myotonia (delayed relaxation of a muscle after a strong contraction) occurring in myotonic muscular dystrophy may be treated with medications such as quinine, phenytoin, or mexiletine, but no actual long term treatment has been found. Occupational therapy assists the individual with MD in engaging in his/her activities of daily living (self-feeding, self-care activities, etc) and leisure activities at the most independent level possible. This may be achieved with use of adaptive equipment or the use of energy conservation techniques. Occupational therapy may implement changes to a person's environment, both at home or work.
53 | P a g e
MUSCULAR DYSTROPHY
SURGICAL TREATMENT
54 | P a g e
MUSCULAR DYSTROPHY
Surgery When contractures become more pronounced, tenotomy surgery may be performed. In this operation, the tendon of the contractured muscle is cut, and the limb is braced in its normal resting position while the tendon regrows. In FSH, surgical fixation of the scapula can help compensate for shoulder weakness. For a person with OPMD, surgical lifting of the eyelids may help compensate for weakened muscular control. For a person with DM, sleep apnea may be treated surgically to maintain an open airway. Scoliosis surgery is often needed in DMD but much less often in other muscular dystrophies. Surgery is recommended at a much lower degree of curvature for DMD than for scoliosis due to other conditions, since the decline in respiratory function in DMD makes surgery at a later time dangerous. In this surgery, the vertebrae are fused together to maintain the spine in the upright position. Steel rods are inserted at the time of operation to keep the spine rigid while the bones grow together. When one muscle pulls much more strongly than its opposing muscle, it may cause the joint to become partially dislocated, which is called subluxation. Tenotomy is also performed to prevent or correct subluxation, especially of the hip joint in cerebral palsy. Chronic pain or bone deformity may prevent a person from moving a joint through its full range of motion, leading to contracture. Contracture also occurs in a variety of neuromuscular diseases, including muscular dystrophies and polio. Degeneration of one muscle can allow the opposing muscle to pull too hard across the joint, shortening the muscle.
55 | P a g e
MUSCULAR DYSTROPHY
Figure no-1.8 shows the Tenotomy
56 | P a g e
MUSCULAR DYSTROPHY
PHYSIOTHERAPY ASSESMENT
57 | P a g e
MUSCULAR DYSTROPHY
PHYSIOTHERAPY ASSESSMENT
SUBJECTIVE:
Name: Age: Sex: Occupation: Address: Present medical history: Chief complaintFamily history: Duration: Onset: gradual/sudden. Affected site: affected parts are noted. Past medical history: About history of vaccinations, History of post infections, History of SMT. History of medical treatment. History of any MMR diseases during birth/childhood. History of drugs.
58 | P a g e
MUSCULAR DYSTROPHY
History of any viral, bacterial infections. Health condition of the members. Position of patient in the family. Any history of associated diseases. Personal history: Habits Routine activities Social history: Socio- economic status Place of living
OBJECTIVE:
On observation: Built of the patient. Position of the eyes. Movements of the chestwall during expiration and inspiration. Any open injuries. Any involuntarymovement of distal parts of the limbs. Any external appliances brace, splints.etc. Check for facial expressions. Any deformity. gait Posture. Normal activities.
59 | P a g e
MUSCULAR DYSTROPHY
On examination: Higher function examination. Level of consciousness. Orientation. Speech. Memory. Identification Behavior. Intelligence. Examination of cranial nerves: (3,4,7 etc.,) 3rd and 4th cranial nerves: (occulomotor and trochlear) Study the patients head and ask to follow an object held arm length-full range of horizontal and vertical movements are noted. When light is shown in to the normal eye, only the pupil on that side consists.
60 | P a g e
MUSCULAR DYSTROPHY
7th cranial nerve: (facial nerve) Abnormal eye movements are noted Asymmetrical elevation of one corner of mouth is noted. Sensory system examination: Superficial: Touch- soft or crude. Pain- Superficial or deep. Temperature- Hot OR Cold. Deep: Joint position. Vibrations. MOTOR EVALUATION: Muscle grading. 0 No activity is noted. 1 Flicker of contraction.(trace) 2 Movement in elimination of gravity-One full range of motion in gravity eliminated position.(poor) 3- movement against gravity-one full range of motion against gravity.(fair) 4- Movements with minimal resistance. one full range of motion against gravity with minimal resistance.(good) 5- Normal- one full range of motion
61 | P a g e
MUSCULAR DYSTROPHY
against gravity with maximal resistance.(normal) Muscle tone Hypotonisity or hypertonicity. Mostly hypotonicity is noted due to peripheral nerve involvement. Muscle girth: Measured by using inch tape
Reflexes: Upper limb (decreased) Biceps Triceps Brachioradialis Lower limb(decreased) Quadriceps Tibialis anterior Plantar response.
Absent (-) Depressed (+) Normal (+ +) Brisk
Brisk with clonusc.) Examination of co-ordination. Co-ordination tests for upper and lower limbs- voluntary activities of limbs are noted.
d.) Examination of status of skin: Pale or scaly.
62 | P a g e
MUSCULAR DYSTROPHY
Examination of ROM: The active and passive range of motion of joints, which are affected, should be assessed. Hip. Knee. Ankle pelvic. Shoulder Elbow Wrist Finger movements are noted.
Examination of gait: High stepping gait.
63 | P a g e
MUSCULAR DYSTROPHY
Difficulties of gait. Parameters of gait are noted. Examination of posture: Check the posture of body in various positions standing, sitting, and lying. Check for scoliosis. Check for kyphosis. Check for lardosis. Examination of respiration: Breathing pattern. Examine diaphragmatic components chest wall expansion Lung function test. Functional assessment: Daily activities are noted Dependent activities are noted.
64 | P a g e
MUSCULAR DYSTROPHY
REHABILITATION
REHABILITATION Rehabilitation is the utilization of existing capacities of the handicapped person by the combined and co-ordinate use of medical, social, occupational, educational and vocational measures to the optimum level of his functional abilities
65 | P a g e
MUSCULAR DYSTROPHY
Muscular Dystrophy Association These are words of belief, relied on by our Muscular Dystrophy Association India. Planted in early 2000, we have blossomed comfort for a large cohort of Muscular Dystrophy community. And of course we have diagnosis and researches done to ease the hold of the disease. With able support from more like minds, things would prove ever positive. Neither so early, nor late as well, the Muscular Dystrophy Association India is one of the very few of its kind in India. Since its first breath on the 5th of February 2000, the association has itself programmed with the duty to help those afflicted by the disease MUSCULAR DYSTROPHY. When the idea of such an association was kindled by Dr. Gunter Schuebraundt on his visit to India, it was Dr. V. Viswanathan, Paediatric Neurologist from KKCTH1, Chennai, Dr. Kalpana Gowrishankar, Geneticist, KKCTH, Mr. Ganapathi and Ms. Kavitha, KKCTH, Mr. V. R. Anil Kumar, Rotary Club (Madras South) and few other personalities with similar frequencies to venture into the thought and realizing what was just an Association all but just in mind.
With the case statistics increasing every now and then, the growing importance on our organization have led us to where we are now. The support group consists of the Patients, Parents, Doctors, Scientists, Volunteers and all of those interested in alleviating the status quo of the situation and who can positively contribute to the affected.
66 | P a g e
MUSCULAR DYSTROPHY
After six long years of experience, involvements and a shift of the Association from its initial base at KKTCH to SMF2, Chennai, in the midway, we have managed to establish a large cohort of Patients, Parents, and Volunteers and like minds from all over South India. All of the patients who have registered with us have been examined in detail and investigated on biochemical and genetic aspect and diagnostic label established Efforts havent stopped with helping the parents and children.The biggest advantage would be meeting the challenges and sharing across culture and borders. We are actively linked with International bodies working to find a cure for the disease. We are one of the chosen centres for the Global programme on Duchenne Muscular Dystrophy called the CINRG3. Basic objectives include, Psychological support to Patients and Parents Dissemination of information on the disease Promote interaction and communication amongst Doctors, Patients, Parents and Scientists Promote Research and Development for these orphan disease Create a National task Force for Public awareness
67 | P a g e
MUSCULAR DYSTROPHY
68 | P a g e
MUSCULAR DYSTROPHY
69 | P a g e
MUSCULAR DYSTROPHY
MEDICAL Members are : Physiatrist Orthopedic surgeon Neurosurgeon Plastic surgeon Psychiatrist Pediatrician Obstretrician Geneticist Neonatologist Rheumatologist Cardiologist Cardiac surgeon General surgeon Oncologist Urologist Ophthalmologist
70 | P a g e
MUSCULAR DYSTROPHY
General physician & Family physician
PARAMEDICAL Physiotherapist Occupational therapist Creative movement therapist Recreational therapist Prosthatist orthotist Rehabilitation nurse Speech pathologist Psychologist Biomedical engineer Music therapist SOCIO VOCATIONAL Social worker Vocational counselor Vocational evaluator Skilled instructor Placement officers
71 | P a g e
MUSCULAR DYSTROPHY
Child development specialist Special educator Employement agencies Some of the most important staff for the muscular dystrophy is 1.Physiotherapist 2. Occupational therapist 3.Rehabilitation nurse 4.Prosthatist orthotist
Physiotherapist:Role: a. To decrease the low back pain b. Maintain the muscle power c. Maintain ROM d. Prevent deformities and contractures e. Nutritional advise to prevent the development of obesity f. Prevent the respiratory muscle complications g. Maintain functional status h. Psychological confidence Occupational therapist: The therapist should help return him to his occupational life and adapt him to daily living
72 | P a g e
MUSCULAR DYSTROPHY
Rehabilitation nurse Those nurses help him to arrange his needs and encourage and motivate the patient in positive way
Prosthatist orthotist:Those doctors will arranges the needed braces and splint to prevent him to contracture and deformities.
73 | P a g e
MUSCULAR DYSTROPHY
PHYSIOTHERAPY MANAGEMENT
74 | P a g e
MUSCULAR DYSTROPHY
PHYSIOTHERAPY MANAGEMENT PROBLEM LIST: Low back pain Decreased muscle power Decreased range of motion Development of contractures and deformities Develop muscle wasting Reduced respiratory muscle strength Development of chest infections Decreased functional status AIMS:1. To decrease the low back pain 2. Maintain the muscle power 3. Maintain ROM 4. Prevent deformities and contractures 5. Nutritional advise to prevent the development of obesity
6.
Prevent the respiratory muscle complications
7. Maintain functional status
75 | P a g e
MUSCULAR DYSTROPHY
Muscular dystrophy patients are in 3 stages 1. Ambulatory stage. 2. Wheel chair stage. 3. Bed ridden stage.
Ambulatory stage
INTERVENTION:-
TO DECREASE LOWBACK PAIN: SWD applied to back to decrease pain Spinal extension exercises should be encouraged to increase strength of muscle Encourage symmentrical sitting for postural correction
TO MAINTAIN MUSCLE POWER By using MMT,strengthening of weakened muscles Most commonly proximal muscles are involved so strengthen the proximal muscles
76 | P a g e
MUSCULAR DYSTROPHY
TO MAINTAIN ROM Active movement and active assisted movements should be encouraged to maintain joint
PNF technique may be useful to increase ROM
TO PREVENT DEFORMITIES AND CONTRACTURES The two joint muscles are most prone to developing significant contractures Early in the course of disease process, a home program must be instituted to include ROM, stretching and positioning
Both parents and child should get the education about the expected changes in muscle balance
How they can pay an active role in preventing or limiting the impact of contractures
Initially encourage the active range of motion exercises If active ROM becomes more difficult, parents should assist the child to move his limbs, to stretch the muscle and particular structures
The stretching program should include static stretching techniques with prolonged mild tenson to affect both visco elastic and plastic properties of muscle.
Positions should encouraged to prevent contractures
77 | P a g e
MUSCULAR DYSTROPHY
Once the child has significant hip flexor or IT band contracture, position the child in a standing frame during several hours helps to provide prolonged stretch to hip knee ankle musculature.
Encourage night splinting to control plantar flexion contracture. Encourage long leg splint at night to prevent knee flexion contracture. By using thoraco lumbo sacral arthosis to prevent kypotic abnormality.
effective bracing minimizes abnormal postures PREVENT RESPIRATORY COMPLICATIONS AND IMROVE RESPIRATORY FUNCTIONS
The child should improve breathing efficiency by the family by teaching breathing exercises
Stressing diaphragmatic breathing Full chest expansion exercises Air shift and rib cage stretching Encourage the child by playing with hand hold incentive Spiro meter units, blowing bobbles and pin wheels.
If there are any secretions accumulated in lungs the family should be taught postural drainage.
IMPROVE FUNCTIONAL STATUS AND MAKE THE INDIVIDUAL FUNCTIONAL INDEPENDENCE
78 | P a g e
MUSCULAR DYSTROPHY
Encourage forced swimming Active and resistive exercise program Low frequency electric stimulation improves the functional status of individual
HOME ADAPTATIONS Rise the height of the bed, chair, toilet so that movement from one place to another place easier.
A boat with firm mattress under it make movement and handling easier Recreational activities include swimming riding TV Games photography ball activities, cycling etc., should be encouraged
Bilateral KAFO use to relax.
WHEEL CHAIR STAGE AND BED BOUND STAGE: Functional Training: Improving mobility function with specific emphasis on improving mobility of axial structures, the head, trunk, hips, and shoulders. Progression to more diffucult motor activates should be gradual. The more severely involved patient may benefit initially from assisted movements progressing to active movements (e.g.; the PNF technique e if R1) to improve initial motor performance. Moving in bed (i.e,. rolling, supine to sit transitions) are essential skills that are often very difficult owing to rigidity and bradykinesia. Sidelyng rolling activities that emphasize segmental rotation patterns (i.e,. isolated upper and
79 | P a g e
MUSCULAR DYSTROPHY
lower trunk rotations) shouyld be practiced rather than a log-rolling pattern. Patients with very stiff trunks may benefit from compensatory rolling strategies using the UE or LE to reach over and initialed the movement (eg DIF patterns of the UE or LE to reach over and initiate the movement (eg DIF patterns of the UE or LE). Sitting posture can be facilitated through exercises designed to improve pelvic mobility as the patient with PD typically sits with a stiff and posterior titled pelvis. Anterior and posterior tilts, side to side tilts, pelvic clock exercises can be practiced while sitting on a therapy ball. These activities can then be progressed to sitting on a stationary surfacce such as a mart table using an inflatable disc to finally no apparatus,
Respiratory Training:
Respiratory dysfunction is linked to morbidity and mortality in patients with MD.
80 | P a g e
MUSCULAR DYSTROPHY
For these patients a comprehensive pulmonary rehabilitation programme should be instituted. Components include diaphragmatic breathing exercises, Air shifting techniques, and exercises that recruited neck, shoulder, and trunk muscles. The patient should be instructed in deep breathing exercises to improve chest wall mobility and vital capacity. Air shifts are promoted to lesser winterer areas of the lung for example basal expansion can be promoted rising manual stretch and resistance to those segments.
Upper body resistance training exercises are indicated. Chest wall mobility can be improved by using PNF UE bilateral symmetrical D2 flexion and extension patterns.
Motor learning stratagies: Walking patterns can be improved with focused instructions of "swing your arms" walk fast or take large steps for the patient with advanced disease and cognitive deficits, repetitive drill like practice should be used. Visual cues inclued stationary floor markings. Dynamic transportable cues.
UE movements were improved by reaching toward a moving target., eg a rolling ball descending down a track. Rhythmic auditory stimulation includes use of a metronome beat or a study beat from musical device.
81 | P a g e
MUSCULAR DYSTROPHY
Pulsed cues to the ear lobe or the hand a form of tacktile cueing.
Group and home exercises:
Group exercises classes can be valuable for patients with MD. The patient can begin in the seated position and progressive standing, using light, touchdown support of the back of the chair. Stretching exercises involving large joints used as initial warm up activites. Well structured low impact aerobics are an appropriate focus for a group class, for eg patient can march in place first in sitting then in standing. Walking with an emphasis on taking large steps high steps. The HEP includes interventions already discussed with exercises designed to improve relaxation mobility, flexibility, strength, and cardiopulmory function.
Standing corner wall stretches can also be used to maintained stretch on upper trunk flexors. Use of cane can be effective in promoting over head motions.
Psychosocial issues
The progressive nature of PD necessitates frequent personal and social adjustments and affects all aspects of life for both patient and family. The principle goal for team members is to assest the patient and family in their understanding of the disease and in developing insides and adjustments that leads to more effective self management.
Feelings of hopelesness and dependency are reduced as patient develops a sense of control over his life.
Patient, family and care giver education:82 | P a g e
MUSCULAR DYSTROPHY
The therapist over all approach needs to be positive and supportive. Community support groups are available for patients and their families. Educate the parents abou the condition and tell the complications regarding the problems which are faced furthers and encourage and motivate to do home exercises which are needed.
Care giver shold encourage the patient to prevent further detoriation.
83 | P a g e
MUSCULAR DYSTROPHY
PROGNOSIS
PROGNOSIS
The prognosis for people with muscular dystrophy varies according to the type and progression of the disorder. Some cases may be mild and progress very slowly over a normal lifespan, while others produce severe muscle weakness, functional disability, and loss of the ability to walk. Some children with muscular dystrophy die in infancy while others live into adulthood with only moderate disability. The muscles affected vary, but can be around the pelvis, shoulder, face
84 | P a g e
MUSCULAR DYSTROPHY
or elsewhere. Muscular dystrophy can affect adults, but the more severe forms tend to occur in early childhood.
85 | P a g e
MUSCULAR DYSTROPHY
SUMMARY
SUMMARY Muscular dystrophies (MD) are inherited disorders characterized by progressive weakness and degeneration of the skeletal or voluntary muscles which control movement, without a central or peripheral nerve abnormality. The muscles of the heart and other involuntary muscles are also affected in some forms of MD, and a few forms involve other organs as well. 10 Types of muscular dystrophy are seen in the world depending upon the part that is involved.
1. 2. 3. 4.
Duchenne muscular dystrophy Becker's muscular dystrophy Congenital muscular dystrophy Distal muscular dystrophy
86 | P a g e
MUSCULAR DYSTROPHY
5. 6. 7. 8. 9. 10.
Emery-Dreifuss muscular dystrophy Facioscapulohumeral muscular dystrophy Limb-girdle muscular dystrophy Myotonic muscular dystrophy Oculopharyngeal muscular dystrophy Spinal muscular atrophy
Among the above types Duchenne muscular dystrophy is the most dangerous. The Beckers is the second most dangerous but the life span of the Duchenne muscular dystrophy is 12-20 but in the Beckers type above 20 years. In the Duchenne muscular dystrophy the patient may die with respiratory complications. No medications are available for muscular dystrophy but research are made to control the disease progression.
BIBLIOGRAPHY
87 | P a g e
MUSCULAR DYSTROPHY
References
1. 2. 3.
1991 Harrison's Principles of Internal Medicine III rd edition. "The muscular dystrophies" III rd edition 1995. 1991 Harrison's Principles of Internal Medicine IV rd edition December 2004
4. 5.
Rehabilitation text Muscular Dystrophy Association. http://ptct.client.shareholder.com/releasedetail.cfm?ReleaseID=448803
6. http://www.parentprojectmd.org/site/ 7. R.M. Lehman & G.L. McCormack, 2001. Neurogenic and Myopathic Dysfunction pp. 802-803.
8.
Guillaume-Benjamin-Armand Duchenne 1987 Neurogenic and Myopathic Dysfunction pp.789.
88 | P a g e
MUSCULAR DYSTROPHY
9.
http://en.wikipedia.org/wiki/Muscular_dystrophy. Dystrophy Campaign Retrieved 9 April 2007.
10. Muscular 11. "The
muscular dystrophies". Lancet 359 (9307): 687695. Institute of Neurological Disoders and Stroke . sequence variations within the 4q35 region are associated with
12. National 13. "Specific
facioscapulohumeral muscular dystrophy".
14. Wyeth
Initiates Clinical Trial with Investigational Muscular Dystrophy
Therapy MYO-029.
15. Muscular
Dystrophy Association's website in Greece 2000.
89 | P a g e
Das könnte Ihnen auch gefallen
- DYSTROPHYDokument15 SeitenDYSTROPHYleeyan2wenty6Noch keine Bewertungen
- Muscular DystrophyDokument3 SeitenMuscular Dystrophyderrickmason626Noch keine Bewertungen
- Duchenne Muscular Dystrophy: Causes, Symptoms & TreatmentsDokument18 SeitenDuchenne Muscular Dystrophy: Causes, Symptoms & TreatmentsLusi MunawarohNoch keine Bewertungen
- Muscular DystrophyDokument33 SeitenMuscular DystrophyNurdina AfiniNoch keine Bewertungen
- Motor Neuron DiseaseDokument8 SeitenMotor Neuron DiseaseyigoNoch keine Bewertungen
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBewertung: 4 von 5 Sternen4/5 (2)
- Assessment of Gait Disorders in ChildrenDokument3 SeitenAssessment of Gait Disorders in ChildrenMadalina RarincaNoch keine Bewertungen
- Cerebral PalsyDokument44 SeitenCerebral PalsyprinceejNoch keine Bewertungen
- Essentials of Research Methodology for Physiotherapy StudentsDokument1 SeiteEssentials of Research Methodology for Physiotherapy StudentsProductivity 100Noch keine Bewertungen
- Cystic Fibrosis Affects Lungs and DigestionDokument2 SeitenCystic Fibrosis Affects Lungs and DigestionYanyan Umpar PologNoch keine Bewertungen
- Surgical Management of Cerebral PalsyDokument72 SeitenSurgical Management of Cerebral PalsySamNoch keine Bewertungen
- DDH Treatment - PFDokument30 SeitenDDH Treatment - PFHendra SantosoNoch keine Bewertungen
- Pediatric OrthopedicsDokument28 SeitenPediatric OrthopedicsEdwin OkonNoch keine Bewertungen
- Spina BifidaDokument16 SeitenSpina BifidaJared Gonzales100% (1)
- EctrodactylyDokument2 SeitenEctrodactylyFrianne LuxNoch keine Bewertungen
- Duchenne Muscular Dystrophy Symptoms, Causes, TreatmentDokument9 SeitenDuchenne Muscular Dystrophy Symptoms, Causes, TreatmentrutwickNoch keine Bewertungen
- Wrist Case Study 1Dokument3 SeitenWrist Case Study 1superhoofy7186100% (2)
- Relieve Back Pain with Protruded Disc TreatmentDokument12 SeitenRelieve Back Pain with Protruded Disc TreatmentElvisNoch keine Bewertungen
- Muscular DystrophyDokument21 SeitenMuscular DystrophyIqra Iftikhar100% (4)
- Rehabilitation for Rheumatic and Musculoskeletal DiseasesDokument42 SeitenRehabilitation for Rheumatic and Musculoskeletal DiseasesNaveen KumarNoch keine Bewertungen
- Spina Bifida: Saba Ramzan Nadia Shoukat Laraib Yasin Anam WarisDokument40 SeitenSpina Bifida: Saba Ramzan Nadia Shoukat Laraib Yasin Anam WarislaraibNoch keine Bewertungen
- Spinal Cord InjuryDokument14 SeitenSpinal Cord Injuryapi-301913778Noch keine Bewertungen
- Juvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDDokument38 SeitenJuvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDLavi GoyalNoch keine Bewertungen
- CP DVTDokument3 SeitenCP DVTBrian O'NeillNoch keine Bewertungen
- Case StudyDokument10 SeitenCase StudyDharitri HaloiNoch keine Bewertungen
- Case 2 Acute Ischemic Stroke wk.6Dokument3 SeitenCase 2 Acute Ischemic Stroke wk.6Nader AbdurasadNoch keine Bewertungen
- Scoliosis: Aka: Idiopathic Scoliosis, Adolescent ScoliosisDokument12 SeitenScoliosis: Aka: Idiopathic Scoliosis, Adolescent ScoliosisLei Coloma SissonNoch keine Bewertungen
- LeprosyDokument9 SeitenLeprosyJohn Ribu Parampil100% (1)
- Cholelithiasis in ChildrenDokument10 SeitenCholelithiasis in ChildrenrendyjiwonoNoch keine Bewertungen
- I. Severe Protein-Energy Malnutrition (PEM) : A. General Considerations On PEMDokument6 SeitenI. Severe Protein-Energy Malnutrition (PEM) : A. General Considerations On PEMReg LagartejaNoch keine Bewertungen
- Case StudyDokument30 SeitenCase StudyNur SolehahNoch keine Bewertungen
- Brittle Bone Disease Causes Fragile BonesDokument30 SeitenBrittle Bone Disease Causes Fragile BonesKhim GoyenaNoch keine Bewertungen
- Bilateral Knee OADokument35 SeitenBilateral Knee OAMu'iz Beatforteen50% (2)
- Malnutrition in Stroke PatientDokument8 SeitenMalnutrition in Stroke PatientFetria MelaniNoch keine Bewertungen
- Colles FractureDokument89 SeitenColles Fracturenur syafiqah kamaruzaman100% (1)
- Myasthenia Gravis BrochureDokument2 SeitenMyasthenia Gravis BrochureMolly100% (1)
- Spinal Cord Injury: Mrs. Zaida ZaracenaDokument36 SeitenSpinal Cord Injury: Mrs. Zaida ZaracenaArdhel LoslosoNoch keine Bewertungen
- Medical & Surgical Management in Cerebral PalsyDokument13 SeitenMedical & Surgical Management in Cerebral PalsySahil SahniNoch keine Bewertungen
- Clubfoot Definition, Types, and TreatmentDokument5 SeitenClubfoot Definition, Types, and TreatmentcrisolandNoch keine Bewertungen
- Combined Cortical SensationsDokument14 SeitenCombined Cortical SensationsDyna MaxNoch keine Bewertungen
- ClubfootDokument5 SeitenClubfootCherry AlmarezNoch keine Bewertungen
- Chapter Eight: Principles, Objectives and General Ap-Proaches Relating To Community-Based RehabilitationDokument5 SeitenChapter Eight: Principles, Objectives and General Ap-Proaches Relating To Community-Based RehabilitationAnandhu GNoch keine Bewertungen
- Cerebral Palsy and EducationDokument14 SeitenCerebral Palsy and EducationDatin Lianawati IdayuNoch keine Bewertungen
- Rheumatoid Arthritis Treatment and Management GuideDokument32 SeitenRheumatoid Arthritis Treatment and Management GuideamirthaNoch keine Bewertungen
- Multiple SclerosisDokument6 SeitenMultiple SclerosisandrearuzziNoch keine Bewertungen
- Pneumonia: Causes, Types, Symptoms & TreatmentDokument5 SeitenPneumonia: Causes, Types, Symptoms & TreatmentudesaoilmillNoch keine Bewertungen
- Spina Bifida OverviewDokument26 SeitenSpina Bifida OverviewPearl Raiza HadaniNoch keine Bewertungen
- Cerebral PalsyDokument7 SeitenCerebral Palsyapi-315294234Noch keine Bewertungen
- Nursing Management of Patient with Ovarian CancerDokument7 SeitenNursing Management of Patient with Ovarian CancerTerrena Lyn BlackmanNoch keine Bewertungen
- Rehabilitation in Spinal Cord InjuryDokument2 SeitenRehabilitation in Spinal Cord InjuryAudry ArifinNoch keine Bewertungen
- Inflammatory Bowel Disease .. Last EditDokument22 SeitenInflammatory Bowel Disease .. Last EditRashed ShatnawiNoch keine Bewertungen
- Leprosy PDFDokument19 SeitenLeprosy PDFsteffiecruz06Noch keine Bewertungen
- Types of Traction and Casts Used in Fracture TreatmentDokument12 SeitenTypes of Traction and Casts Used in Fracture TreatmentNoemi Nazareno MarceloNoch keine Bewertungen
- Type 2 DiabetesDokument5 SeitenType 2 DiabetesNuno Sa PunsoNoch keine Bewertungen
- Dysphagia ManagementDokument21 SeitenDysphagia ManagementSooraj A. O.100% (1)
- ArthritisDokument18 SeitenArthritisGEETA MOHAN100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Appendicitis: The Etiology, Hygenic and Dietetic TreatmentVon EverandAppendicitis: The Etiology, Hygenic and Dietetic TreatmentBewertung: 3 von 5 Sternen3/5 (2)
- Ayurvedic Treatment of Muscular DystrophyDokument9 SeitenAyurvedic Treatment of Muscular DystrophyMukesh JainNoch keine Bewertungen
- Born With Four Wheels: Muscular DystrophyDokument11 SeitenBorn With Four Wheels: Muscular DystrophyJohanNoch keine Bewertungen
- General Questions and Possible AnswersDokument21 SeitenGeneral Questions and Possible AnswersDeepak PathaniaNoch keine Bewertungen
- Neurology NotesDokument87 SeitenNeurology Notesvijay1234568883100% (1)
- BellDokument79 SeitenBellvijay1234568883Noch keine Bewertungen
- Intruduction PagesDokument24 SeitenIntruduction Pagesvijay1234568883Noch keine Bewertungen
- Allergic AsthmaDokument99 SeitenAllergic Asthmavijay1234568883Noch keine Bewertungen
- Akula Abhinay ResumeDokument4 SeitenAkula Abhinay Resumevijay1234568883Noch keine Bewertungen
- Periarthritis ShoulderDokument76 SeitenPeriarthritis Shouldervijay1234568883Noch keine Bewertungen
- Hanuman ChalisaDokument10 SeitenHanuman Chalisavijay1234568883Noch keine Bewertungen
- BronchiectasisDokument71 SeitenBronchiectasisvijay1234568883Noch keine Bewertungen
- Pa Tell EctomyDokument69 SeitenPa Tell Ectomyvijay1234568883Noch keine Bewertungen
- BellDokument79 SeitenBellvijay1234568883Noch keine Bewertungen
- BellDokument79 SeitenBellvijay1234568883Noch keine Bewertungen
- TKRDokument8 SeitenTKRvijay1234568883Noch keine Bewertungen
- Gait AssessmentDokument4 SeitenGait Assessmentvijay1234568883Noch keine Bewertungen
- Year Planner 2011Dokument1 SeiteYear Planner 2011vijay1234568883Noch keine Bewertungen
- FasciculationDokument7 SeitenFasciculationvijay1234568883Noch keine Bewertungen
- Gait AssessmentDokument4 SeitenGait Assessmentvijay1234568883Noch keine Bewertungen
- 1Dokument1 Seite1vijay1234568883Noch keine Bewertungen
- Understand TSGLI BenefitsDokument2 SeitenUnderstand TSGLI BenefitsJoseph LawerenceNoch keine Bewertungen
- Soap Making: Borax (NaDokument15 SeitenSoap Making: Borax (Naa aNoch keine Bewertungen
- اللائحة التنظيمية لسفن الكروز - النسخة العربية - TransDokument10 Seitenاللائحة التنظيمية لسفن الكروز - النسخة العربية - TranssalsabilNoch keine Bewertungen
- Bangladesh National Building Code 2012 Part 07 - Construction Practices and SafetyDokument83 SeitenBangladesh National Building Code 2012 Part 07 - Construction Practices and SafetyPranoy Barua100% (3)
- 01 Basic Design Structure FeaturesDokument8 Seiten01 Basic Design Structure FeaturesAndri AjaNoch keine Bewertungen
- PKL Geri RevDokument3 SeitenPKL Geri RevKurniati NiaNoch keine Bewertungen
- TVL ICT IllustrationNCII Q1Module2Dokument12 SeitenTVL ICT IllustrationNCII Q1Module2Kimberly Trocio Kim100% (1)
- DSI-DYWIDAG Geotechnics Rock Bolts enDokument6 SeitenDSI-DYWIDAG Geotechnics Rock Bolts enTomás Nunes da SilvaNoch keine Bewertungen
- Natalia Mooting QDokument1 SeiteNatalia Mooting QPok Nik LiNoch keine Bewertungen
- Commodity FuturesDokument19 SeitenCommodity FuturesPrabhu G UmadiNoch keine Bewertungen
- New Haven Harbor Connecticut Navigation Improvement Project Integrated Feasibility Report and Environmental Impact StatementDokument23 SeitenNew Haven Harbor Connecticut Navigation Improvement Project Integrated Feasibility Report and Environmental Impact StatementHelen BennettNoch keine Bewertungen
- ITC's diverse businesses: cigarettes, packaging, hotels, paperboards, stationery, matches, incense sticks, retail, food, exportsDokument1 SeiteITC's diverse businesses: cigarettes, packaging, hotels, paperboards, stationery, matches, incense sticks, retail, food, exportsShashank JainNoch keine Bewertungen
- Simonson 20033wDokument15 SeitenSimonson 20033wbahrul.hidayah@yahoo.comNoch keine Bewertungen
- Piling Procedure - IoclDokument8 SeitenPiling Procedure - IocltpgggkNoch keine Bewertungen
- Compact Dehumidifier Fluted Flat Bed - FFB Series: Technical Data SheetDokument4 SeitenCompact Dehumidifier Fluted Flat Bed - FFB Series: Technical Data SheetLê ĐạtNoch keine Bewertungen
- ClindamycinDokument1 SeiteClindamycinTanalie Dulawan100% (3)
- Aquatic Ecology and LimnologyDokument96 SeitenAquatic Ecology and LimnologySale AlebachewNoch keine Bewertungen
- CX-5 BX-10 No. 1 & 1.5 Fluid Cylinder PartsDokument5 SeitenCX-5 BX-10 No. 1 & 1.5 Fluid Cylinder PartsPierreNoch keine Bewertungen
- READING MODULE 4 - CompressedDokument13 SeitenREADING MODULE 4 - CompressedPaolo IcangNoch keine Bewertungen
- Original Instruction Manual: Hypro Series 9303Dokument24 SeitenOriginal Instruction Manual: Hypro Series 9303vandoNoch keine Bewertungen
- KitchenAid 5ksm150psDokument18 SeitenKitchenAid 5ksm150psFrancisco AlvarezNoch keine Bewertungen
- Stakeholders in The Iep Process JDokument9 SeitenStakeholders in The Iep Process Japi-546526887Noch keine Bewertungen
- Solarizer Value, Spring & UltraDokument4 SeitenSolarizer Value, Spring & UltraEmmvee SolarNoch keine Bewertungen
- Crosbys Molasses and MoreDokument37 SeitenCrosbys Molasses and MoreShaikh MeenatullahNoch keine Bewertungen
- Ravi ProjectDokument92 SeitenRavi ProjectAvinash Avii100% (1)
- Calcul BADokument15 SeitenCalcul BAHanane BenGamraNoch keine Bewertungen
- Msae Msae2018-Arwm012 Full Dronespraying 2Dokument4 SeitenMsae Msae2018-Arwm012 Full Dronespraying 2Muhammad Huzaifah Mohd RoslimNoch keine Bewertungen
- Rtaa SB 4 - 10011991Dokument6 SeitenRtaa SB 4 - 10011991alcomech100% (3)
- A7V Variable Displacement PumpDokument22 SeitenA7V Variable Displacement PumpEduardo CramerNoch keine Bewertungen
- PositionsDokument4 SeitenPositionsMixsz LlhAdyNoch keine Bewertungen